CHAPTER 84 Percutaneous Discectomy
INTRODUCTION
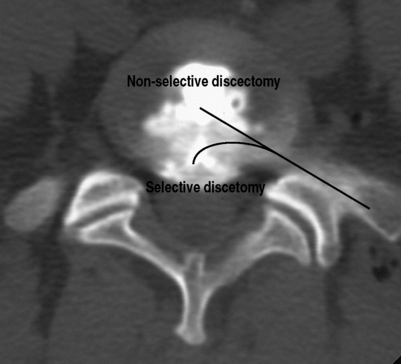
Percutaneous discectomy is a method for treating disc herniations. There are two basic types of percutaneous discectomy: selective and nonselective.1 The goal of a selective percutaneous discectomy is to remove disc from the posterior third of the disc space, where herniations reside.1 This is typically accomplished with surgical instruments and/or lasers which can be placed in the disc with an endoscope and then directed to the area of the herniation under direct vision. As such, it is a true surgical procedure, and will not be discussed further in this chapter. The goal of a nonselective discectomy is to remove nucleus from the center of the disc, relying on the accompanying changes in disc mechanics to effect a change in the herniation (Fig. 84.1).
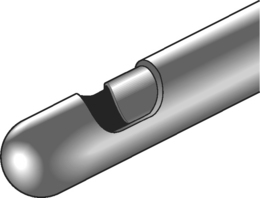
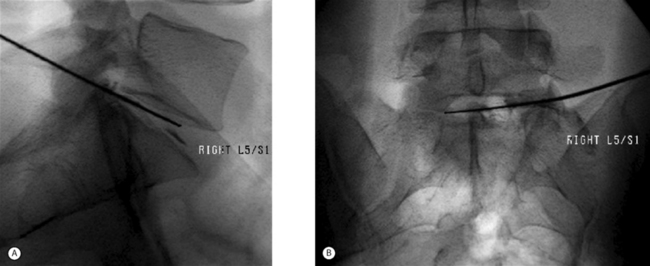
The original device used to perform a nonselective percutaneous discectomy was the nucleotome (Fig. 84.2). This device functions as a mechanical shaver which is placed into the center of the disc under fluoroscopic guidance, and nucleus is then aspirated. While other devices have largely supplanted the nucleotome, the objective of the procedure remains nonselective removal of nucleus from the disc. As all the devices used for nonselective discectomy are placed using fluoroscopy, without incisions or surgical instruments (Fig. 84.3), in contemporary practice the procedure is commonly done by interventional spine physicians and radiologists as well as by surgeons.
EVOLUTION OF PERCUTANEOUS DISCECTOMY
The driving force behind the development of percutaneous discectomy was the series of neurological catastrophes that occurred with the use of chymopapain in the United States in the 1970s.1 Chemonucleolysis with chymopapain was introduced into clinical practice in 1964 by Lyman Smith.2 In the years since, it has been demonstrated in randomized controlled trials to be an effective treatment for sciatica due to disc herniation.3 Unfortunately, due to technical errors by some practitioners, chymopapain was injected into the subarachnoid space of a number of patients who developed severe neurological deficits, leading it to be removed from the US market in 1985, although it continued to be available in other parts of the world. The prevailing theory on the mechanism of action of chymopapain at the time was that it relieved nerve root pressure due to disc herniation by ‘internally decompressing’ the disc; that is, by decreasing intradiscal pressure it reduced mechanical tension on a bulging anulus and relieved nerve root compression.4
Onik, who introduced the nucleotome, postulated that decreasing intradiscal pressure by mechanical means would have the same therapeutic effect as chymopapain, while avoiding the dangers associated with chymopapain.5 Subsequent biomechanical studies confirmed that percutaneous discectomy resulted in a decrease in intradiscal pressure.6 Percutaneous discectomy with the nucleotome, which became known as automated percutaneous lumbar discectomy (APLD), was adopted with considerable enthusiasm. This enthusiasm seemed justified by early, nonrandomized studies, which yielded 70–75% success rates in treating patients with sciatica due to a disc herniation with very low complication rates.7,8 However, controlled studies, one comparing APLD to chemonucleolysis and the other to microdiscectomy, demonstrated considerably lower success rates of 29–37%.9,10 By the latter part of the 1990s, APLD had fallen out of favor in much of the world, although there continue to be areas, most notably Italy, where it is still commonly performed.
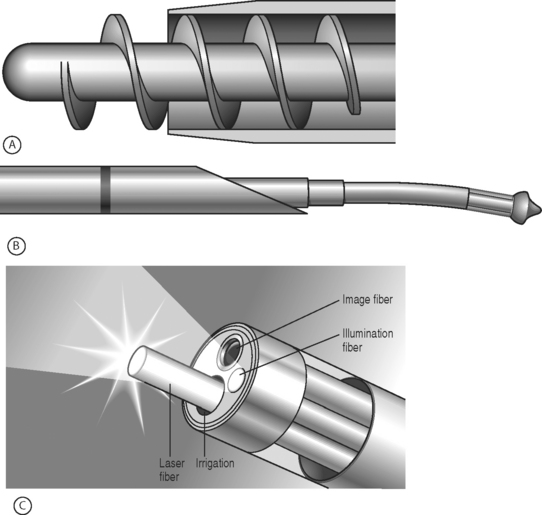
Recently, there has been a resurgence of interest in percutaneous discectomy, coinciding with the introduction of new devices for doing the procedure (Fig. 84.4). These devices are all considerably smaller than the nucleotome and are therefore easier to insert. The Dekompressor device is similar to the nucleotome in that it removes tissue mechanically, while both the Lase device and the Arthrocare spine wand vaporize tissue, the Lase device with laser and the Arthrocare device with a low-temperature process known as coblation. As there are no controlled studies available on the efficacy of these devices, at this point it is not possible to determine whether they represent an advance over percutaneous discectomy done with the nucleotome.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


