2 in. stockinette
2 in. cast padding
TABLE 7-1 Acceptable Parameters for Closed Treatment of Pediatric Distal Radius Fractures
Age in Years
Coronal Alignment
Sagittal Alignment
Reference
<5
Up to 35 degrees
Lovell and Winter
5-12
Up to 25 degrees
>12
Up to 15 degrees
4-9
15 degrees
15-20 degrees
Rockwood and
9-11
5 degrees
10-15 degrees
Wilkins
11-13
0 degree
10 degrees
>13
0 degree
0-5 degrees
4-9
5-10 degrees
15-20 degrees
Bae
Data from Bae DS. Pediatric distal radius and forearm fractures. J Hand Surg Am. 2008;33(10):1911-1923; Waters PM, Bae DS. Fractures of the distal radius and ulna. In: Beaty JH, Kasser JR, eds. Rockwood and Wilkin’s Fractures in Children. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010:292; Skaggs DL, Frick S. Upper extremity fractures in children. In: Weinstein SL, Flynn JM eds. Lovell and Winter’s Pediatric Orthopaedics. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:1760.
2-in. fiberglass
Large basin
Room temperature water
Scissors
Nonsterile gloves
Apply stockinette to injured limb leaving 1 to 2 in. of extra length proximally and distally from where cast will ultimately end.
Apply two to three layers of cast padding evenly without wrinkles (material should overlap previous layer by 50% and be rolled to avoid excessive tightness) (Video 7-1).
Stop cast padding distally at level of distal palmar crease to permit full metacarpophalangeal joint flexion.
Stop cast padding proximally at proximal third of forearm for short arm casts and proximal third of arm for long arm casts (ensure elbow is flexed to 90 degrees for long arm casts) (Fig. 7-1).
Dunk fiberglass in room temperature water, and squeeze some but not all of the excess water out.
Apply fiberglass in similar manner as cast padding (Video 7-2) (during the fiberglass application, fold back the excess stockinette to ensure no rough edges of fiberglass are against the skin).

FIGURE 7-1 Application of cast underpadding. Note the elbow is flexed 90 degrees and the cast underpadding stops of the level of the distal palmar flexion crease to permit full digital motion. (Courtesy of Joshua M. Abzug, MD.)
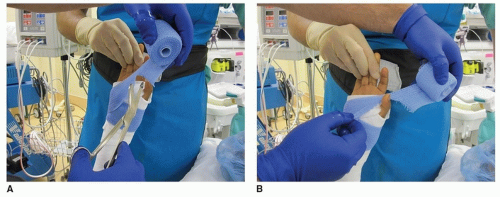
FIGURE 7-2 A. Application of the fiberglass cast material around the thumb by cutting the fiberglass. B. Stretching of the fiberglass around the thumb to permit full thumb range of motion following cast application. (Courtesy of Joshua M. Abzug, MD.)
Mold cast utilizing a three-point or interosseous mold.
Full thumb motion should be present (Fig. 7-2).
Closed treatment with or without a closed reduction is the most common treatment for pediatric distal radius fractures.
Ensure proper cast application technique utilizing small-sized cast padding and fiberglass.
Use only two to three layers of cast padding, each overlapping the previous layer by 50%.
Assess alignment 3 to 5 days following a closed reduction and again 1 week later to ensure maintenance of alignment.
Remove cast utilizing in-out technique with a blade that is not dull to avoid burns and/or lacerations.
Related posts:
 Operative Treatment of Pediatric Forearm Fractures Using Flexible IM Rodding
Operative Treatment of Pediatric Forearm Fractures Using Flexible IM Rodding
 Percutaneous Fixation of Slipped Capital Femoral Epiphysis
Percutaneous Fixation of Slipped Capital Femoral Epiphysis
 Calcaneal Lengthening Osteotomy
Calcaneal Lengthening Osteotomy
 Proximal Tibial Osteotomy for Tibia Vara
Proximal Tibial Osteotomy for Tibia Vara
 Anterior Spinal Fusion for Thoracolumbar Idiopathic Scoliosis
Anterior Spinal Fusion for Thoracolumbar Idiopathic Scoliosis
 Derotation of the Scoliotic Spine
Derotation of the Scoliotic Spine
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


