3 Pathological and other abnormal gaits
In order for a person to walk, the locomotor system must be able to accomplish four things:
1. Each leg in turn must be able to support the body weight without collapsing
2. Balance must be maintained, either statically or dynamically, during single leg stance
3. The swinging leg must be able to advance to a position where it can take over the supporting role
4. Sufficient power must be provided to make the necessary limb movements and to advance the trunk.
Specific gait abnormalities
The following sections are based on a manual of lecture notes for student orthotists published by New York University (1986). Despite being over 25 years old, the manual includes a very useful list of common gait abnormalities, all of which can be identified by eye, which still hold today. The manual criticises the common practice of identifying gait abnormalities by their pathological cause, for example ‘hemiplegic gait’, which immediately suggests that all hemiplegics walk in the same way, which is far from true, and also neglects the changes in gait which may occur with the passage of time, or result from treatment. The manual suggests that it is preferable to use purely descriptive terms, such as ‘excessive medial foot contact’. This practice will be adopted in the following sections. Some of the gait abnormalities described in the New York University publication apply only to the gait of subjects wearing orthoses; these descriptions have been omitted from the present text.
1. The subject has no choice, the movement being ‘forced’ on them by weakness, spasticity or deformity
2. The movement is a compensation, which the subject is using to correct for some other problem, which therefore needs to be identified.
Lateral trunk bending
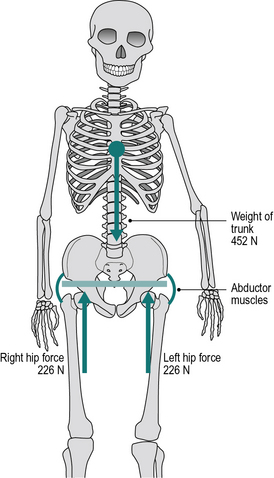
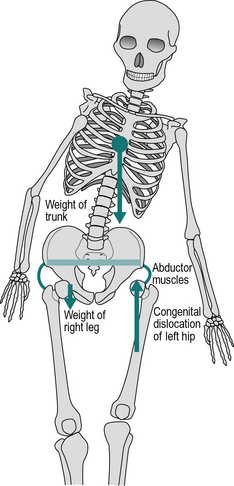
In the examples which follow, the weight of the trunk is 452 N, corresponding to a mass of 46 kg, and the weight of the right leg is 147 N, corresponding to a mass of 15 kg. As explained in Chapter 1 (p. 000), weight is a force, calculated by multiplying an object’s mass by the acceleration due to gravity, 9.81 m/s2.
Figure 3.1 shows a schematic of the trunk, pelvis and hip joints when standing on both legs. The abductor muscles are inactive and the weight of the trunk is divided equally between the two hip joints. Figure 3.2 shows what happens in a normal individual when the right foot is lifted off the ground: the force through the left hip joint increases by a factor of six, from 226 N (23 kgf or 51 lbf) to 1510 N (154 kgf or 339 lbf). This increase in force is made up of three components:
1. The whole of the weight of the trunk is now supported by the left hip joint, instead of being shared between the two hips which produces an anti-clockwise moment
2. The weight of the right leg is now taken by the left hip instead of by the ground, which also produces an anti-clockwise moment
3. The left hip abductors (primarily gluteus medius) contract, produces a clockwise moment to keep the pelvis from dropping on the unsupported side. The reaction force to this contraction passes through the left hip.
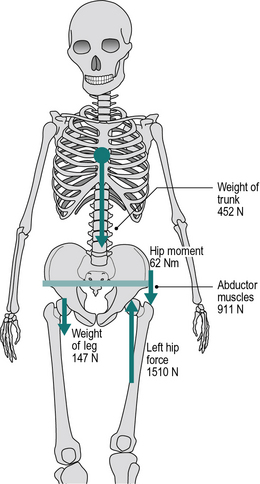
These three components contribute to the increased force in the left hip as follows:
• The force from the trunk increases from 226 N to 452 N (23 kgf or 51 lbf) as this is now not shared
• Weight of right leg: 147 N (15 kgf or 33 lbf)
• Contraction of abductors: 911 N (93 kgf or 204 lbf)
The four conditions which must be met if this mechanism is to operate satisfactorily are:
• The absence of significant pain on loading
• Adequate power in the hip abductors
• A sufficiently long lever arm for the hip abductors
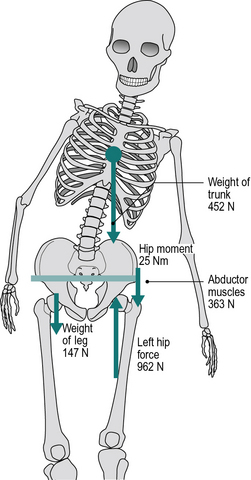
The effect of lateral trunk bending on the joint force is shown in Figure 3.3. There is no effect on components (1) and (2) of the increased force, but if the centre of gravity of the trunk is moved directly above the left hip, this eliminates the anti-clockwise moment produced by the mass of the trunk. The abductors are now only required to contract with a force of 363 N (37 kgf or 81 lbf) to balance the anti-clockwise moment provided by the weight of the right leg. There is thus a reduction of 548 N (56 kgf or 123 lbf) in the abductor contraction force and a corresponding reduction in the total joint force, from 1501 N down to 962 N. The numbers in the illustrations refer to standing; during the stance phase of walking, higher forces are to be expected due to the vertical accelerations of the centre of gravity, which cause the force transmitted through the leg to fluctuate above and below body weight (see Fig. 2.19). However, these fluctuations tend to be less in pathological than in normal gait, since the vertical accelerations are less in someone walking with a shorter stride length. The numbers also suppose that the bending of the trunk brings its centre of gravity exactly above the hip joint. This is unlikely to happen in practice, of course, but the principles remain the same, whether the centre of gravity is not deviated as far as the hip joint or even if it passes lateral to it.
There are a number of conditions in which this gait abnormality is adopted.
1. Painful hip:
If the hip joint is painful, as in osteoarthritis and rheumatoid arthritis, the amount of pain experienced usually depends to a very large extent on the force being transmitted through the joint. Since lateral trunk bending reduces the total joint force, ‘Trendelenburg gait’ is extremely common in people with arthritis of the hip. Although it produces a useful reduction in force and hence in pain, the forces still remain substantial (962 N in Fig. 3.3) and some form of definitive treatment is usually required.
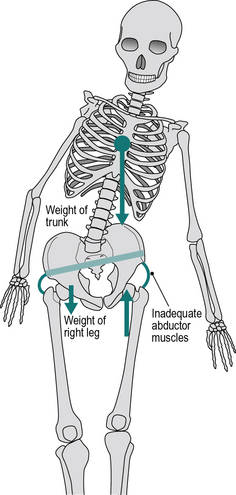
2. Hip abductor weakness:
If the hip abductors are weak, they may be unable to contract with sufficient force to stabilise the pelvis during single leg stance. In this case, the pelvis will dip on the side of the foot which is off the ground (Trendelenburg’s sign, as opposed to ‘Trendelenburg gait’). In order to reduce the demands on the weakened muscles, the subject will usually employ lateral trunk bending, in both standing and walking, to reduce joint moment as far as possible (Fig. 3.4). Hip abductor weakness may be caused by disease or injury affecting either the muscles themselves or the nervous system which controls them.
3. Abnormal hip joint:
Three conditions around the hip joint will lead to difficulties in stabilising the pelvis using the abductors: congenital dislocation of the hip (CDH, also known as developmental dysplasia of the hip), coxa vara and slipped femoral epiphysis. In all three, the effective length of the gluteus medius is reduced because the greater trochanter of the femur moves proximally, towards the pelvic brim. Since the muscle is shortened, it is unable to function efficiently and thus contracts with a reduced tension. In CDH and severe cases of slipped femoral epiphysis, a further problem exists in that the normal hip joint is effectively lost, to be replaced by a false hip joint, or pseudarthrosis. This abnormal joint is more laterally placed, giving a reduced lever arm for the abductor muscles, and it may fail to provide the ‘solid and stable fulcrum’ required. The combination of reduced lever arm and reduced muscle force gives these subjects a powerful incentive to walk with lateral trunk bending (Fig. 3.5). In many cases, particularly in older people with CDH, the false hip joint becomes arthritic and they add a painful hip to their other problems. Pain is frequently also a factor in slipped femoral epiphysis.
4. Wide walking base:
If the walking base is abnormally wide, there is a problem with balance during single leg stance. Rather than tip the whole body to maintain balance, as in Figure 2.28A, lateral bending of the trunk may be used to keep the centre of gravity of the body roughly over the supporting leg. In most cases, this will need to be done during the stance phase on both sides, leading to bilateral trunk bending and a waddling gait. A number of conditions, which will be described later, may cause a wide walking base.
Anterior trunk bending
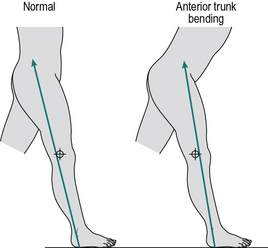
One important purpose of this gait pattern is to compensate for an inadequacy of the knee extensors. The left panel of Figure 3.6 shows that early in the stance phase, the line of action of the ground reaction force vector normally passes behind the axis of the knee joint and generates an external moment which attempts to flex it. This is opposed by contraction of the quadriceps, to generate an internal extension moment. If the quadriceps are weak or paralysed, they cannot generate this internal moment and the knee will tend to collapse. As shown in the right panel of Figure 3.6, anterior trunk bending is used to move the centre of gravity of the body forwards, which results in the line of force passing in front of the axis of the knee, producing an external extension (or hyperextension) moment. In addition to anterior trunk bending, subjects will sometimes keep one hand on the affected thigh while walking, to provide further stabilisation for the knee.
Other causes for anterior trunk bending are equinus deformity of the foot, hip extensor weakness and hip flexion contracture (Perry, 1992).
Posterior trunk bending
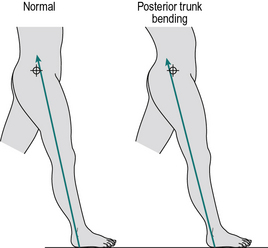
One form of posterior trunk bending is essentially a reversed version of anterior trunk bending, in that early in the stance phase, the whole trunk moves in the sagittal plane, but this time backwards instead of forwards. Again, it is most easily observed from the side. The purpose of this is to compensate for ineffective (weak) hip extensors. The line of the ground reaction force early in the stance phase normally passes in front of the hip joint (Fig. 3.7, left panel). This produces an external moment which attempts to flex the trunk forward on the thigh and is opposed by contraction of the hip extensors, particularly the gluteus maximus. Should these muscles be weak or paralysed, the subject may compensate by moving the trunk backwards at this time, bringing the line of action of the external force behind the axis of the hip joint, as shown in the right panel diagram of Figure 3.7.
Increased lumbar lordosis
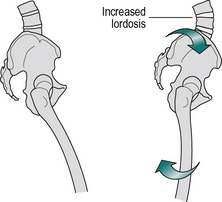
The most common cause of increased lumbar lordosis is a flexion contracture of the hip. It is also seen if the hip joint is immobile due to ankylosis. Both of these deformities cause the stride length to be very short, by preventing the femur from moving backwards from its flexed position. This difficulty can be overcome if the femur can be brought into the vertical (or even extended) position, not through movement at the hip joint but by extension of the lumbar spine, with a consequent increase in the lumbar lordosis (Fig. 3.8).
Functional leg length discrepancy
Four gait abnormalities (circumduction, hip hiking, steppage and vaulting) are closely related, in that they are designed to overcome the same problem – a functional discrepancy in leg length. A review on the topic of leg length discrepancy was published by Gurney (2002).
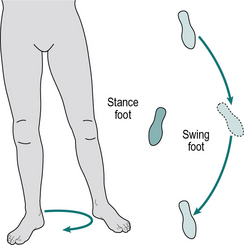
Circumduction
Ground contact by the swinging leg can be avoided if it is swung outward, in a movement known as circumduction (Fig. 3.9). The swing phase of the other leg will usually be normal. The movement of circumduction is best seen from in front or behind. Circumduction may also be used to advance the swinging leg in the presence of weak hip flexors, by improving the ability of the adductor muscles to act as hip flexors while the hip joint is extended.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


