Supramalleolar Osteotomy for Realignment of the Ankle Joint
Keywords
• Supramalleolar osteotomy • Focal dome osteotomy • Ankle deformity • Deformity planning • Ankle Arthritis • Ankle realignment • Ankle malalignment • Distal tibial ostetotomy
Introduction
Distal tibia and ankle deformities are complex because rarely are these deformities uniplanar and without sequelae. These deformities are challenging and can lead to impaired ankle/foot mechanics, which result in osteoarthritis, pain, and dysfunction. Supramalleloar osteotomy of the distal tibia is used to realign the ankle and foot to the leg, thus improving function while preserving articular integrity of the ankle and relieving pain.1–3 Supramalleolar osteotomy is an extraarticular procedure that realigns the mechanical axis, thereby restoring ankle function.1,4 The procedure is versatile and can address uniplanar and oblique plane deformities due to osteoarthritis, malunited ankle/pilon fractures, malunited ankle fusions, and congenital and developmental deformities.1–3,5–9 This osteotomy can address ankle procurvatum/recurvatum, varus/valgus, internal/external rotation, equinus, calcaneus, and limb length discrepancy. Clinical and radiographic preoperative planning is critical to identify the level and magnitude of deformity. The goal of this article is to outline the indications/contraindications, clinical evaluation, radiographic preoperative planning, surgical technique, and postoperative care.
Indications for Supramalleolar Osteotomies
Supramalleolar osteotomies may be indicated for the following problems:
Osteoarthritis
Osteoarthritis of the ankle has been shown to occur from malalignment of the ankle joint.1,2,4–6,14 Malalignment results in uneven distribution of forces, which can lead to early wear of the articular surface and degenerative changes in the ankle.1,15 Ramsey and Hamilton16 in their posttraumatic ankle fracture experiments concluded that lateral talar displacement by 1 mm reduces the tibiotalar contact area by 42%. Similarly, Tarr and colleagues21 reported further evidence of the effects of malalignment of the distal tibia and decrease in tibiotalar contact. Other factors such as inadequate subtalar joint inversion/eversion, ligamentous laxity, and muscle imbalance can further contribute to unequal loading of the ground reaction forces about the ankle joint. Supramalleolar osteotomy will realign the malaligned ankle joint, thus equally distributing the forces on the joint. Realignment, through osteotomy, improves ankle joint mechanics and slows the progression of osteoarthritis.
In cases of severe osteoarthritis with a concomitant malalignment of the ankle or distal tibia, salvage of the ankle may not be possible with supramalleolar osteotomy alone. In such instances, supramalleolar realignment followed by total ankle replacement has been reported in the literature.17,18 Also, for ankle joint preservation, a supramalleolar osteotomy followed by hinged external fixation ankle distraction has been reported.19,20
Malunited distal tibia
Malunions of the distal tibia are common complications of traumatic injury. These deformities make ambulation difficult and frequently require surgical intervention. Deformities greater then 15° in the distal tibia can decrease the tibiotalar contact area by 42%.21 Unequal forces on the mortise result in pain and advance the deterioration of the ankle joint. Malunions can occur in the sagittal, frontal, transverse, or oblique plane and increase abnormal loading on the ankle joint and the lower extremity.1
Sagittal plane deformity
Procurvatum or recurvatum deformity occurs in the sagittal plane and is best visualized on a standing lateral radiograph (Fig. 1A–D). Compensation for the deformity is by ankle joint plantar flexion or dorsiflexion. Because there is less ankle joint dorsiflexion available, procurvatum deformities are not tolerated as well as recurvatum deformities. Patients with procurvatum also complain of ankle joint impingement because of limited ankle joint dorsiflexion, whereas those with recurvatum have less plantar flexor strength at push off. This foot position does not maximize the arc of motion within the ankle and creates unequal load on the articular surfaces. When revising this malposition, it is necessary to convert the motion that is present into a more functional arc. Soft tissue contractures of the ankle and subtalar capsule, along with a tight heel cord may need to be addressed. The release of these structures assists in improving the motion of the foot and ankle. The compensatory soft tissue contractures are discussed in greater detail later in this article.
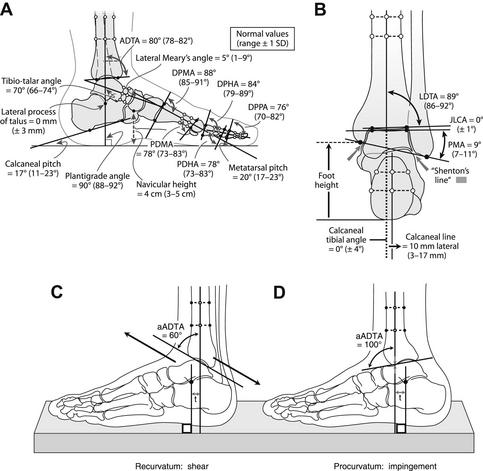
One must maintain axial alignment in the sagittal plane. Anterior or posterior translation of the foot with respect to the distal tibia, such that the middiaphyseal line of the tibia passes through the lateral process of the talus, allows the foot to function anatomically (see Fig. 1A–D). When this line is posterior to the lateral process of the talus, the foot becomes longer, thus increasing the lever arm on the foot, making walking more difficult.
Frontal plane deformity
A frontal plane deformity is characterized by varus or valgus malunions of the ankle or distal tibia. Malalignment in the frontal plane of the ankle joint is best evaluated on a standing anterior-posterior radiograph. Normally, varus malalignment does not result in degeneration of the ankle joint because of the buttressing effect of the medial malleolus. The wide medial malleolus and the medial talar facet articulation serve to maintain the contact area and the dispersion of forces between the tibia and talus (Fig. 2A). However, varus malalignment does create problems in the subtalar joint and first ray, which can become symptomatic and painful. Normally, the subtalar joint compensates for varus malalignment of the ankle through subtalar eversion. However, if compensatory subtalar joint motion is not present, the forefoot compensates by plantarflexing the first ray. The plantar flexion of the first ray increases the arch and decreases the weightbearing surface area of the foot.1
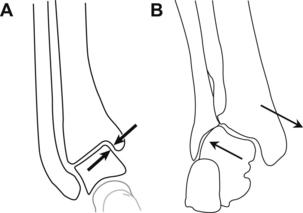
The valgus ankle leads to degeneration of the ankle joint (see Fig. 2B). During normal single leg stance, the ground reaction force vector passes lateral to the ankle and subtalar joint and imparts a valgus thrust on those joints. In a valgus ankle, there is increased load on the lateral tibiotalar surfaces because of increased lateralization of the ground reaction vector (GRV). Chronic loading of the ankle in this manner can disrupt the tibial-fibular articulation and lead to disruption of the syndesmosis, lateral translation of the talus in the ankle mortise, and degeneration of the articular surfaces of the tibia and talus.
Congenital and developmental deformities
Congenital and developmental deformities, such as clubfoot, cerebral palsy, fibular hemimelia, Charcot-Marie-Tooth, myelomeningocele, amongst others can cause deformity that is resistant to correction. These deformities can significantly affect the ankle joint complex. Supramalleolar osteotomy has been used successfully to treat resistant congenital deformities22,23 and aims to realign the foot to the leg and create a plantigrade foot.
Internal/external rotation
Tibial torsion deformities are most common in childhood and normally resolve spontaneously.23 Symptomatic medial and lateral torsion deformities that do not resolve by 8 years of age may require tibial derotation osteotomy. The osteotomy to correct rotational deformity is made in the distal tibial metaphysis. After correction is achieved, fixation with smooth Steinman pins protects the physis. Typically, only severe or symptomatic rotational deformities are addressed with a supramalleolar osteotomy. However, rotational deformities that are present in combination with osseous malalignment are addressed simultaneously in the distal tibia.
Clinical presentation
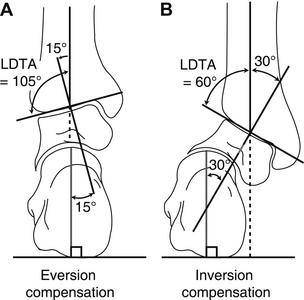
During the physical examination, it is important to note painful areas of the foot and ankle. Supramalleolar deformities can occur at the level of the ankle or juxta-articular, which may induce ankle instability. In such cases, a clinical stress of the ankle (talar tilt and anterior draw) should be performed. Ankle varus deformity is tolerated less well when there is adequate subtalar joint motion because the subtalar joint generally has less eversion compensation available than inversion (Fig. 3A).1 However, in ankle varus deformity, lateral column pain due to subfibular impingement is a common physical examination finding and may require additional osseous procedures.4 Ankle valgus deformities are tolerated well because there is greater inversion compensation available at the subtalar joint (see Fig. 3B).1,24 However, these patients may complain of pain at the subtalar joint or develop first ray symptoms if compensation is not available. The compensatory mechanisms of the foot, as they relate to various ankle deformities, are discussed later in greater detail.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


