Chapter 3. Orthopaedic anatomy
By the end of this chapter you should:
• Be able to identify different types of joint in the body.
• Understand collagen and its function and how this relates to motion/wear.
• Understand the effect of muscles on fractures and the displacement caused.
• Be aware of neurovascular injuries and know which nerves are commonly injured and where.
Joints
Types of joint
First, remember that synovial joints are just one type of joint and that the fibrous and cartilaginous types are just as important.
Synovial joints
The shoulder, elbow, hip, knee and ankle are all synovial joints lined by synovium, which secretes synovial fluid. The articular surfaces are covered with smooth hyaline articular cartilage and movement is determined by the shape of the bones, ligaments, surrounding soft tissues and the joint capsule, which contains the proprioceptors which form the afferent segment of postural reflexes.
Synovial joints can be classified according to shape and the movement that occurs between the bones. Ball and socket joints such as the hip (Fig. 3.1) and shoulder allow movement in all planes, but a hinge joint such as the knee allows movement in one plane only. Condyloid joints such as the radiocarpal joint are elliptical and allow movement in two planes, whereas pivot, or peg, joints such as the superior radioulnar and atlantoaxial joints allow movement about one axis only (Fig. 3.2).
 |
| Fig. 3.1 A ball and socket joint. The ball of the femoral head is enclosed by the cup of the acetabulum. |
 |
| Fig. 3.2 A peg joint. The atlas can pivot on the axis. |
Some joints, such as the patellofemoral joint, have a very large range of movement (Fig. 3.3), but others have much less. The small bones of the tarsus, for example, are linked by plane joints with so little movement that groups of joints must work together to permit a useful range of motion.
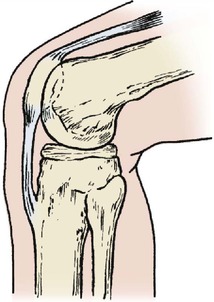 |
| Fig. 3.3 The knee is a hinge joint but the patellofemoral joint is a sliding joint. |
The posterior intervertebral, or facet, joints are also plane joints, as is the sacroiliac joint.
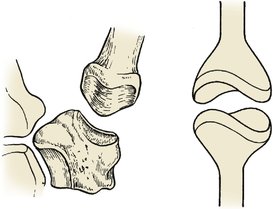
Other joints are more complex and more interesting mechanically. The first carpometacarpal joint is saddle-shaped and similar to a universal joint in design (Fig. 3.4). Other joints work in pairs, including the superior and inferior radioulnar joints, which function as a single unit with two bones moving about an axis that passes through the centre of each (Fig. 3.5). The tibiofibular joints are similar; movement of the ankle produces movement at the superior tibiofibular joint (try it on your own leg). The subtalar joint also consists of two separate articulations between the same two bones, one convex upwards and the other convex downwards, but movement occurs about an oblique axis which does not pass through the articular surface of either.
 |
| Fig. 3.4 A ‘universal’ joint. The first carpometacarpal joint has two saddle-shaped joint surfaces. |
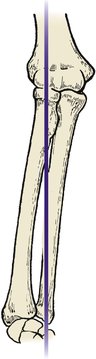 |
| Fig. 3.5 Paired joints. The axis of pronation and supination of the forearm runs through the proximal and distal radioulnar joints. |
Cartilage joints
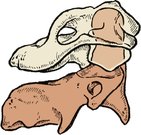
There are two types of cartilage joints: primary, or synchondroses, and secondary, or symphyses (Fig. 3.6). Synchondroses link immature growing bone at the epiphyses in children and have no movement. Symphyses, which are only found in the midline of the body, have a mass of fibrocartilage linking the bones instead of a synovial cavity. The pubic symphysis is the best known but the intervertebral joints with their intervertebral discs and the manubriosternal joint are also symphyses.
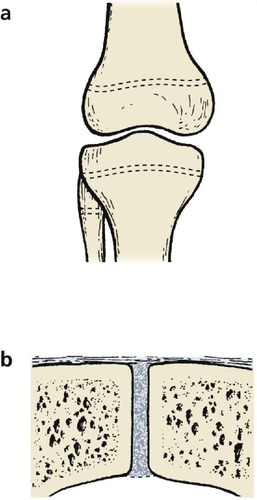 |
| Fig. 3.6 Cartilage joints. (a) Synchondroses at the growing ends of long bones; (b) a symphysis between the two halves of the pubis. |
Fibrous joints
The flat bones of the skull are linked at the suture lines by fibrous tissue, which prevents any appreciable movement. These linkages are, strictly speaking, joints, but their function is to limit movement rather than encourage it. The inferior tibiofibular joint is the largest syndesmosis in the body and is important for the stability of the ankle (Fig. 3.7).
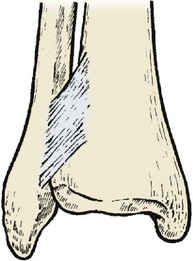 |
| Fig. 3.7 The tibiofibular syndesmosis allows a very slight, but important, degree of movement between the two bones. |
Bones
Types of bone (Fig. 3.8)
Long bones
The epiphysis in a growing long bone is separated from the hollow shaft, or diaphysis, by the epiphyseal plate, or physis. The part of the diaphysis next to the physis is the metaphysis. Any bone arranged like this is called a long bone, even if it is quite short – the phalanges of the fingers and toes are ‘long’ bones in structure. Damage to a growing epiphysis causes deformity.
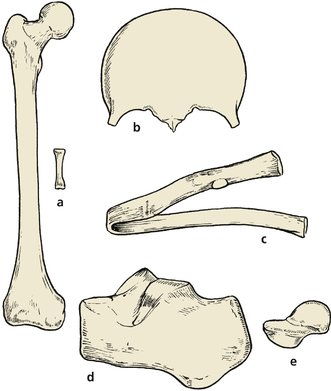 |
| Fig. 3.8 Different types of bone: (a) long bones; (b), (c) flat bones; (d), (e) short bones. |
Flat bones
Flat bones, such as the skull, pelvis and ribs, form in condensations of fibrous tissue and are often called membrane bones. Their function is the protection of soft viscera such as the brain and lungs.
Short bones
Short square bones like those of the tarsus and carpus form in blocks of cartilage and ossify from the centre. They do not have epiphyses.
Accessory ossicles
In addition to the normal bones, accessory ossicles occur as variants of normal. These are entirely innocent structures but can be mistaken for fractures and treated as such. The os trigonum behind the talus (Fig. 3.9a) and the accessory navicular (Fig. 3.9b) are among the most common.
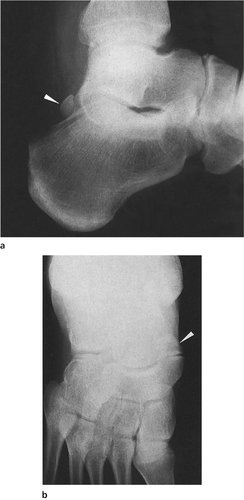 |
| Fig. 3.9 Accessory ossicles: (a) the os trigonum: (b) accessory navicular bone. |
Epiphyses
Growth of bones
Long bones grow from a physis (epiphyseal plate or growth plate) at each end. Although both ends grow, one will generally grow faster than the other and different epiphyses contribute different amounts to the length of a bone.
The lower femoral and upper tibial epiphyses contribute roughly 60% of limb length, but the proximal humeral epiphysis is responsible for 80% of the length of the humerus. The exact proportions need only be remembered by orthopaedic surgeons.
If all growth is stopped at an epiphyseal plate, the limb will be straight but shorter than normal. If only one side of the plate is stopped, which can happen after a fracture through the growth plate, an unpleasant angular deformity may follow (p. 102 and p. 218). These problems do not occur in membrane or cartilage bones, which grow by getting gradually bigger in all directions.
Generalized illness in childhood can retard bone growth and leave a dense line on the radiograph that remains throughout life (growth arrest). These lines are called Harris’ lines and are of no clinical importance (Fig. 3.10).
 |
Fig. 3.10
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
