Operative Treatment of Lesser and Greater Arc Injuries
Rick Tosti
Joseph J. Thoder
DEFINITION
The carpus is a complex, intercalated system of dual rows that allow paired motion within the radial-ulnar and flexion-extension planes. A disruption of the intrinsic ligaments of the carpus or a combination of ligamentous and osseous structures leads to a spectrum of injuries ranging from “wrist sprains” to complex perilunate injuries including lesser and greater arc injuries.11,12,15
Lesser arc injuries are purely capsuloligamentous.
Greater arc injuries have associated carpal fractures.
Disruptions of the normal kinematics and stability of the carpal rows lead to a predictable pattern of posttraumatic degenerative changes.
ANATOMY
The carpus is composed of eight bones arranged in two rows that articulate with the five metacarpals distally and the radius and ulna proximally.
Complex, three-dimensional motion occurs with wrist movement: radial deviation and wrist dorsiflexion are paired, as are ulnar deviation and wrist volar flexion.
Motion is passively transmitted through crossing tendons and guided by bony geometry and ligamentous architecture, which also confer stability.
Volar extrinsic ligaments are oriented in a double V arrangement, with a relative weakness between these V’s called the space of Poirier.
The dorsal extrinsic ligaments provide less structural stability and include the radiotriquetral and dorsal intercarpal (DIC) ligaments (FIG 1B).
The intrinsic ligaments are direct intercarpal connections that provide intrarow stability.
In the proximal row, these include the lunotriquetral interosseous ligament (LTIL) and the scapholunate interosseous ligament (SLIL).
PATHOGENESIS
A high-energy axial load is applied to the thenar eminence causing hyperextension, ulnar deviation, and intercarpal supination. The energy dissipates in a radial to ulnar direction and places the volar structures under tension and the dorsal structures under compression and shear.
Lesser arc injuries are purely ligamentous and advance through four progressive stages as originally described by Mayfield et al14 (FIG 2A):
Stage I: the scapholunate ligament
Stage II: the space of Poirier
Stage III: the UTCC and lunotriquetral ligament
Stage IV: lunate dislocation
Greater arc injuries proceed in the same direction but involve fractures through the radial styloid, scaphoid, lunate, capitate, triquetrum, and ulna, either solely or in combination (FIG 2B).3,10 The prefix “trans” is given to the fractured carpal bone (eg, trans-scaphoid perilunate fracture-dislocation).
A perilunate dislocation describes a dorsal dislocation of the capitate and surrounding carpus, but the lunate remains in
the fossa of the distal radius (FIG 3A,B). Volar dislocations of the carpus are rare (FIG 3C).
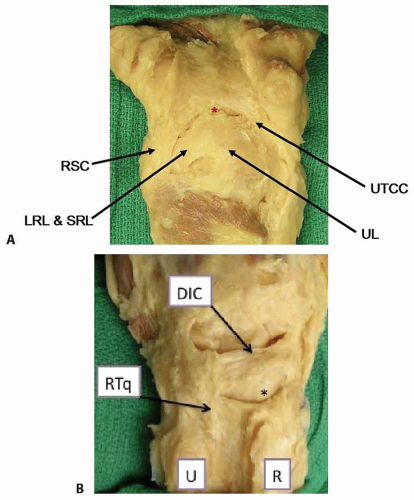
FIG 1 • A. Volar extrinsic carpal ligaments. LRL, long radiolunate ligament; SRL, short radiolunate; RSC, radioscaphocapitate ligament; UL, ulnolunate ligament; UTCC, ulnotriquetrocapitate complex; asterisk, space of Poirier. B. Dorsal extrinsic carpal ligaments. RTq, radiotriquetral ligament; DIC, dorsal intercarpal ligament; asterisk, scaphoid; U, ulna; R, radius.
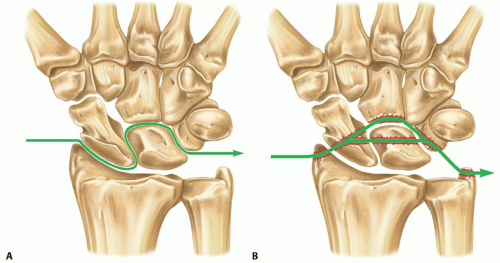
FIG 2 • A. Lesser arc injury. Progression of capsuloligamentous injury from radial to ulnar direction. B. Greater arc injury. Trans-scaphoid perilunate injury pattern.
A lunate dislocation describes a more severe progression in which the capitate translocates into the lunate fossa and displaces the lunate volarly into the carpal tunnel (FIG 3D-F).
As the lunate is ousted through the space of Poirier, a semilunar rent is created in the volar capsule that extends medially and laterally between the V ligaments.
 FIG 3 • A-C. Herzberg stage I: perilunate dislocation. A. Anteroposterior (AP) projection demonstrates loss of lines of Gilula. B. Dorsal dislocation of the capitate. C. Volar dislocation of the capitate (rare). D-F. Herzberg stage II: lunate dislocation. D. AP demonstrating loss of lines of Gilula and a triangular shape of the lunate. E. Stage IIA: volar dislocation of the lunate into the carpal tunnel, with the capitate articulating in the radial fossa. F. Stage IIB: volar dislocation with greater than 90 degrees of rotation. |
NATURAL HISTORY
Missed injuries may occur in up to 25% of cases.8
Common sequelae of untreated injuries include pain, weakness, stiffness, acute carpal tunnel syndrome, flexor tendon rupture, early degenerative joint disease, and wrist instability.11,12,15
Typical instability patterns include scapholunate advanced collapse, scaphoid nonunion advanced collapse, and volar or dorsal intercalated segmental instability.
PATIENT HISTORY AND PHYSICAL FINDINGS
High-energy injuries (fall from height, motor vehicle collision, or sports injuries) are generally causative.
Physical examination findings depend on severity of injury and the elapsed time from injury to presentation.
Stiffness, tenderness, crepitus, swelling, and resistance to motion are common findings. Deformity is usually minimal.
Depending on the severity of injury, the findings can be subtle and easily missed. The examiner must maintain a high index of suspicion.
A thorough neurologic examination is critical. Acute compression of the median nerve may be present in 16% to 46% of cases and is more frequently associated with lunate dislocations.15
If median nerve symptoms are present, serial examinations are necessary to distinguish between nerve contusion (static findings) and nerve compression (progressive findings).
Palpation of radial and ulnar styloids or the individual carpal bones in a greater arc injury may reveal tenderness over specific fractures.
Specific testing of intrinsic and extrinsic ligaments (eg, the Watson test, the lunotriquetral shuck, and the ulnar catch up) may prove difficult and of little value in an acute setting.
IMAGING AND OTHER DIAGNOSTIC STUDIES
True posteroanterior (PA) and true lateral radiographs should be obtained. The diagnosis is made primarily with these views. Equivocal cases may be compared with identical radiographs of the uninjured wrist.
The lines of Gilula are disrupted on the PA view.6
If the SLIL is disrupted, widening of the intercarpal joint or a flexed scaphoid (cortical ring sign) may be seen on the PA view, whereas an abnormal scapholunate interosseous angle (normal 30 to 60 degrees) may be seen on the lateral view.
As the capitate migrates proximally, carpal height may be lost (normal carpal-metacarpal height ratio is >0.5) on the PA view. The concentricity of “the 3 C’s,” representing the distal radius, lunate, and capitate, is lost on the lateral view.
As the lunate displaces and rotates volarly, it appears triangular in shape, as opposed to trapezoidal, on the PA view. The “spilled tea cup” sign describes this appearance on the lateral radiograph, which can be quantified by the radiolunate angle (normal <15 degrees).
Oblique views may help delineate carpal fractures in greater arc injuries. Scaphoid fractures are most common. Capitate, lunate, and triquetral fractures have been described. Fractures of the radial and/or ulnar styloids may also be present.
Other views such as radial-ulnar deviation, flexion-extension, supinated, and clenched fist views are often difficult to obtain and are of little additional value.
Computed tomography may be useful for preoperative assessment in greater arc injuries.
Magnetic resonance imaging (MRI), arthrography, arthroscopy, and bone scan are not indicated in the acute setting after major trauma to the wrist.
DIFFERENTIAL DIAGNOSIS
Wrist sprain
Degenerative joint disease
Isolated intrinsic ligament disruption
Radiocarpal dislocationRelated posts:
 Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
Dorsal Block Pinning of Proximal Interphalangeal Joint Fracture-Dislocations
Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
Dorsal Block Pinning of Proximal Interphalangeal Joint Fracture-Dislocations

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


