Open Scapholunate Ligament Repair and Augmentation
Loukia K. Papatheodorou
Alexander H. Payatakes
Alex M. Meyers
Dean G. Sotereanos
DEFINITION
Scapholunate instability is the most common form of carpal instability.
Scapholunate interosseous ligament (SLIL) injury can result in a predictable pattern of arthritis over time: scapholunate advanced collapse (SLAC).14
Acute tears (<6 weeks from injury) versus chronic tears (>6 weeks from injury)
Acute tears tend to be amenable to primary ligament repair.
Chronic tears tend to require ligament reconstruction or stabilization procedures.
Static or dynamic instability
Static instability: Any or all of the five characteristic changes are present on standard plain radiographs (see in the following text).
Dynamic instability: Normal plain radiographs; however, with loaded (grip view) plain radiographs, any or all of the five characteristic changes may become present.12
Fixed versus reducible deformity
Fixed deformity: The static radiographic changes are not passively correctible.
Reducible deformity: The static radiographic changes are passively correctible.
This distinction may be determined preoperatively by noting improvement in the static changes on plain radiographs of the wrist in radial deviation compared with anteroposterior (AP) views of the wrist.
PATIENT HISTORY AND PHYSICAL FINDINGS
Typical presentation follows a fall onto an outstretched hand with acute onset of wrist pain and mild dorsal wrist swelling.
Key physical examination findings are reviewed in Chapter 67.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Plain radiographs may reveal five characteristic findings suggestive of SLIL pathology (FIG 1).
Scapholunate separation (“Terry Thomas sign”): asymmetric gap between the scaphoid and lunate of more than 3 mm on posteroanterior (PA) radiograph
Cortical ring sign: Ring-shaped cortical hyperdensity and scaphoid foreshortening is seen on PA radiograph as the scaphoid moves into increasing flexion.2
Angular changes in the carpal rows
Scapholunate angle: Normal is 30 to 60 degrees (mean 46 degrees); with SLIL injury, more than 60 degrees is suspicious but more than 70 degrees is considered pathognomic.7
Capitolunate angle: Normal is −15 to 15 degrees (mean 0 degree); with SLIL injury, more than 15 degrees.
Radiolunate angle: Normal is −10 to 10 degrees (mean 0 degree); with SLIL injury, more than 10 degrees (lunate tilted dorsally).
Triangular lunate: As the lunate moves into extension, it assumes a more triangular appearance on PA radiograph (normally the lunate appears more quadrangular). This corresponds to the dorsal tilt noted on the lateral view.
Disruption of Gilula arcs: In the normal wrist, the proximal and distal aspect of the proximal row form gentle concentric arcs. These lines may be disrupted with SLIL tears as the normal relationships between the bones of the proximal row are lost.5
Arthrography: sensitivity 56%, specificity 83%, accuracy 60%15
False-positive results have been documented with communication of contrast shown in asymptomatic patients.2
Computed tomography (CT) arthrography: sensitivity 86% to 100% (100% sensitive in the detection of dorsal ligament tears), specificity 50% to 79% (79% specific in the detection of dorsal ligament tears), accuracy 78% to 83%10
Magnetic resonance imaging (MRI): sensitivity 25% to 60%, specificity 77% to 100%, accuracy 64% to 78%11
Specifically, palmar tears of the SLIL were identified with a sensitivity of 60% and specificity of 77% in a cadaveric
study. However, the more important stabilizing dorsal portion tears were seen in zero of nine specimens.10
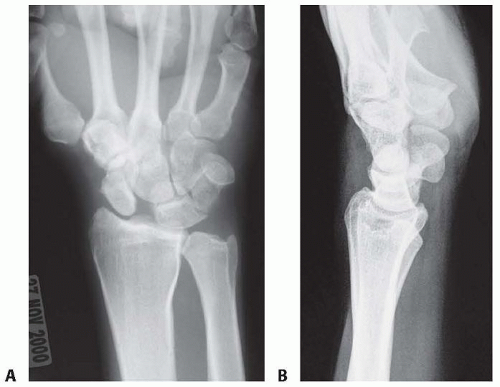
FIG 1 • AP (A) and lateral (B) plain radiographs of a patient with scapholunate ligament tear.
Ultrasound: sensitivity 46%, specificity 100%, accuracy 89%3
A negative result with various imaging studies does not prove an absence of ligamentous injury. Arthroscopy remains the gold standard for the diagnosis of SLIL tears.
DIFFERENTIAL DIAGNOSIS
Dynamic SLIL instability or partial SLIL tear
Radiocarpal arthritis
Scaphoid fracture or nonunion
Keinböck or Preiser disease
NONOPERATIVE MANAGEMENT
Nonoperative management is rarely successful in treating dynamic or static acute scapholunate ligament injuries.
In one study, 0 of 19 patients with dynamic instability treated with immobilization, nonsteroidal anti-inflammatories, and activity modification had substantial reduction in symptoms even up to 12 weeks into treatment.16
SURGICAL MANAGEMENT
Indications
Wrist pain with an acute tear (<6 weeks)
These patients may or may not have static radiographic changes.
If static radiographic changes are present, plain radiographs in radial deviation may show if the radiographic changes are fixed (and therefore are not amenable to soft tissue repair or reconstruction) or reducible in radial deviation (and therefore are amenable to soft tissue repair or reconstruction).
Wrist pain with dynamic instability
The authors advocate diagnostic arthroscopy before open treatment.
Preoperative Planning
General or regional anesthesia
Equipment
Mini suture anchors (1.5 to 2.0 mm)
Kirschner wire driver and smooth wires (0.045 and 0.062 inch)
Arthroscopic equipment (see Chap. 67)
Mini C-arm
A preoperative examination of both wrists is performed and documented, noting passive range of motion, swelling, and the Watson scaphoid shift test.
Positioning
The patient is positioned supine with a hand table.
The bed is rotated 90 degrees so that the hand table extends away from the anesthesia team.
The arthroscopy tower should be placed adjacent to the feet of the patient and be clearly visible to the surgeon.
The mini C-arm should be free to move in and out from the opposite corner perpendicular to the patient.
An upper arm tourniquet should be placed.
The operative arm is prepared and draped. Slack is left in the arm board portion of the drape to allow the sterile wrist traction tower to slide under the arm above the elbow.
The operative wrist is suspended in a wrist traction tower with appropriate traction.Related posts:
 Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
 Fragment-Specific Fixation of Distal Radius Fractures
Fragment-Specific Fixation of Distal Radius Fractures
 Dislocations and Chronic Volar Instability of the Thumb Metacarpophalangeal Joint
Dislocations and Chronic Volar Instability of the Thumb Metacarpophalangeal Joint
 Arthroscopic and Open Triangular Fibrocartilage Complex Repair
Arthroscopic and Open Triangular Fibrocartilage Complex Repair
 Synovectomy of the Elbow
Synovectomy of the Elbow
 Surgical Treatment of Septic Arthritis in the Hand and Wrist
Surgical Treatment of Septic Arthritis in the Hand and Wrist

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


