Open Reduction and Internal Fixation of Radial Head and Neck Fractures
Yung Han
George Frederick Hatch III
John M. Itamura
DEFINITION
Radial head and neck fractures are the most common elbow fractures in adults representing 33% of elbow fractures.
They may occur in isolation or with concurrent osseous, osteochondral, and/or ligamentous injuries.
Management (which involves nonoperative, open reduction internal fixation [ORIF], fragment excision, radial head excision, or radial head replacement) is aimed at restoring motion or both motion and stability to the elbow and forearm, depending on the pattern of injury. This chapter focuses on the decision-making principles and operative techniques for ORIF of radial head and neck fractures.
ANATOMY AND BIOMECHANICS
The radial head is entirely intra-articular with two articulations: (1) radiocapitellar joint and (2) proximal radioulnar joint (PRUJ).
The radiocapitellar joint has a saddle-shaped articulation allowing flexion, extension, and forearm rotation.
The PRUJ, constrained by the annular ligament, allows rotation of the radial head in the lesser sigmoid notch of the proximal ulna.
To avoid creating a mechanical block to pronation and supination, implants must be limited to a 90-degree arc (the “safe zone”) outside the PRUJ (FIG 1).7
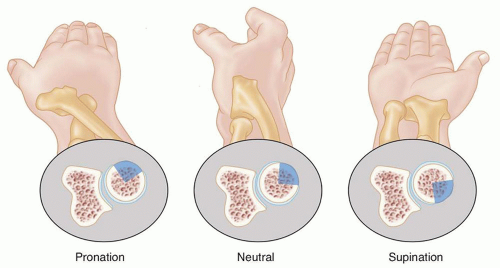
FIG 1 • The safe zone is a roughly 90-degree arc of the radial head that does not articulate with the ulna in the PRUJ with full supination and pronation. With the wrist in neutral rotation, the safe zone is anterolateral.
There is considerable variability in the shape of the radial head, from nearly round to elliptical, as well as variability in the offset of the head from the neck.14
Blood supply to the radial head is tenuous with a major contribution from a single branch of the radial recurrent artery in the safe zone and minor contributions from both the radial and interosseous recurrent arteries which penetrate the capsule at its insertion into the neck (FIG 2).26
The anterior band of the medial collateral ligament (MCL) is the primary stabilizer to valgus stress. The radial head, a secondary stabilizer, maintains up to 30% of valgus resistance in the native elbow. Therefore, in cases where the MCL is ruptured:
A radial head that is not reparable should be replaced with a prosthesis and not excised given its biomechanical importance.
It may be prudent to protect a repaired radial head from high valgus stress during early range of motion.
The radial head also functions in the transmission of axial load, transmitting 60% of the load from the wrist to the elbow.21 This is a crucial consideration when the interosseous membrane is disrupted in the Essex-Lopresti lesion.9 Resection of the radial head in this setting results in devastating longitudinal radioulnar instability, proximal migration of the radius, and possible ulnar-carpal impingement.
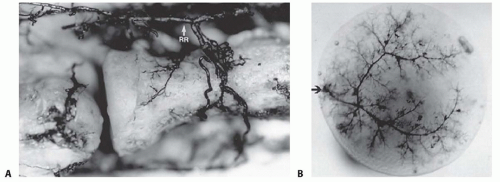 FIG 2 • A. The radial recurrent artery, a branch of the radial artery, provides the main blood supply to the radial head. B. In most cadaveric specimens, a branch of the radial recurrent penetrates the radial head in the safe zone. (From Yamaguchi K, Sweet FA, Bindra R, et al. The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am 1997;79[11]:1653-1662.) |
PATHOGENESIS
Radial head fractures result from trauma. A fall on an outstretched hand with the elbow in extension and the forearm in pronation produces an axial or valgus load (or both) driving the radial head into the capitellum, fracturing the relatively osteopenic radial head.2
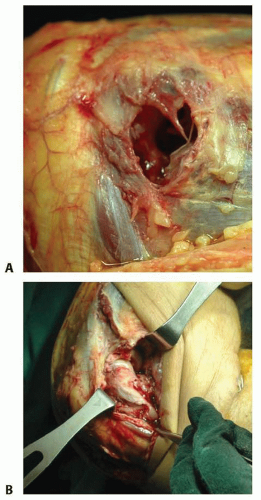
FIG 3 • Soft tissue injuries occur with unstable radial head fractures. Sample pictures showing (A) large capsular rupture and (B) avulsion of the lateral collateral ligament (LCL) and common extensor tendons from the lateral epicondyle.
Nondisplaced or minimally displaced injuries do not usually have associated injuries. However, displaced, comminuted, or unstable fractures have a high association of soft tissue injuries (FIG 3) that can lead to considerable complications, including pain, arthrosis, instability, and disability:
Capitellar cartilage defects, capitellar bone bruises, and/or posterior dislocation can occur with radial head fractures.
Axial loading may also rupture the interosseous membrane causing longitudinal radioulnar instability with dislocation of the distal radioulnar joint (DRUJ) (Essex-Lopresti fracture). An impacted radial neck or depressed radial head fracture should be highly suspicious of a concomitant interosseous membrane and DRUJ injury (FIG 4).
The “terrible triad” injury results from valgus loading of the elbow, disrupting the MCL or lateral ulnar collateral ligament, and fracturing the radial head and coronoid process.
Radial head fractures can also occur with proximal ulnar fractures (Monteggia fracture) (FIG 5).
 FIG 4 • AP x-ray showing a depressed articular fracture with impaction at the radial neck. This fracture pattern is highly suspicious for an Essex-Lopresti fracture. Radial head replacement is recommended. If ORIF is performed, the DRUJ should be stabilized to prevent instability. |
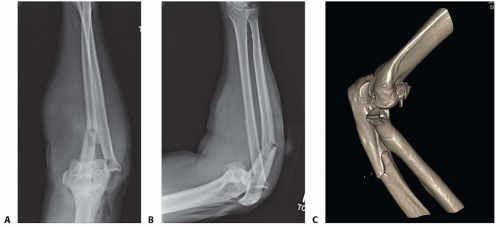 FIG 5 • A,B. AP and lateral x-ray showing a type II Monteggia fracture—posterior dislocation of radial head (or fracture) and proximal ulnar fracture with posterior angulation. C. CT scan clearly showing impaction fracture of the radial head that may not be appreciable on x-ray. |
NATURAL HISTORY
Type I Fractures
Nondisplaced and offer no block to pronation and supination on examination
Represents approximately 82% of radial head fractures18
Nonoperative treatment generally results in good to excellent outcomes with minimal loss of motion or resultant arthrosis.1,3,8,12
Stiffness due to capsular contracture is the main reason for a poor outcome; however, it can often be managed successfully with physical therapy.
Type II Fractures
Displaced marginal segments that can block normal forearm rotation. According to Broberg and Morrey,6 the fragment should be greater than or equal to 30% of the articular surface and be displaced greater than or equal to 2 mm. We only include fractures with three or fewer articular fragments, which meet criteria for fractures that can be operatively reduced and fixed with reproducibly good results.
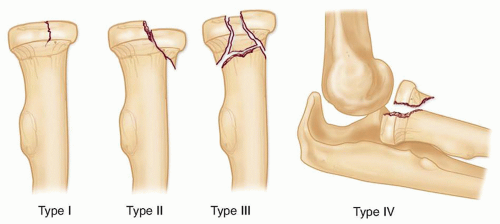
FIG 6 • The modified Mason classification for radial head fractures.
Represents approximately 14% of radial head fractures18
Earlier studies suggested nonoperative treatment or radial head excision as the standard treatment,13,19,20,23 but as knowledge and technology advanced, optimal treatment has become more controversial.
Greater than 2 mm of displacement has often been cited as an indication for ORIF, but good results have been obtained in studies treating 2 to 5 mm of displacement nonoperatively.1,12
A mechanical block is the only clear indication for surgery.
A recent meta-analysis16 found successful nonoperative treatment in 80% compared to successful ORIF treatment in 93% for stable Mason type II fractures; however, the authors concluded that there was insufficient evidence to recommend optimal treatment.
Complications from nonoperative treatment such as painful clicking, nonunion, and arthrosis can be treated with radial head excision or arthroplasty; however, it is considered with modest increase in function. It has shown 23% fair or poor results at 15 years of follow-up.5
Type III Fractures
Comminuted or impacted articular fractures (see FIG 4) are optimally managed with prosthetic replacement.
Represents approximately 3% of radial head fractures18
Radial head arthroplasty or excision is considered when satisfactory reduction or stable fixation is not obtained or in comminuted fractures because fixation of a radial head with more than three articular fragments is fraught with poor results.22Related posts:
 Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures
Fragment-Specific Fixation of Distal Radius Fractures
Vascularized Bone Grafting and Capitate Shortening Osteotomy for Treatment of Kienböck Disease
Operative Treatment of Metacarpal Fractures
Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures
Fragment-Specific Fixation of Distal Radius Fractures
Vascularized Bone Grafting and Capitate Shortening Osteotomy for Treatment of Kienböck Disease
Operative Treatment of Metacarpal Fractures

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


