CHAPTER 19 Open bony augmentation of glenoid bone loss—iliac crest and allograft—surgical technique





Introduction
The consequence of anterior glenoid bone loss in shoulder instability is well known. Some degree of bone loss exists in most recurrent anterior shoulder instability; however, it has been reported to exist in up to 22% of patients after an initial dislocation.1–3 Burkhart and DeBeer4 found that significant anterior glenoid bone loss results in failure of arthroscopic stabilization procedures, and they advocate open reconstruction of the defect using a coracoid process bone graft. Several authors have described methods to quantify bone loss3,5; however, the technique presented by Gerber and Nyffeler6 is our preference for deciding whether or not to augment the glenoid during preoperative planning. These authors determined that 70% less force was required to dislocate the humeral head from the glenoid when the length of the glenoid bony defect was more than the maximum radius of the glenoid (Fig. 19-1).
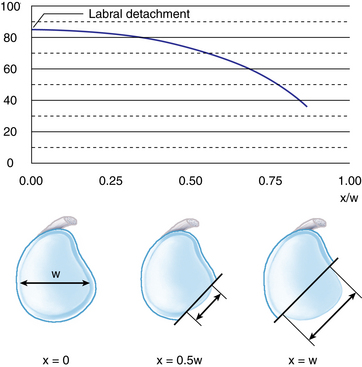
(Redrawn from Gerber C et al: Classification of glenohumeral joint instability. Clin Orthop Relat Res 400:65–76, 2002.)
Although the long-term effects of these alternatives have yet to be determined, Warner et al demonstrated that placing the autogenous tricortical iliac crest bone graft intra-articularly appears to have a high rate of union and stability.7 In addition, the study revealed satisfactory subjective outcomes, and all patients returned to sports participation. Recently, Provencher8 described another technique of reconstructing the anterior glenoid deficiency with the use of distal tibia allograft bone. The authors reported excellent outcomes in all three patients treated with the method and described this operation as not only avoiding the potential complications of coracoid transfer but also claiming it to anatomically restore the articular surface of the glenoid.
Preoperative history, examination, and radiographic findings
Radiographic findings
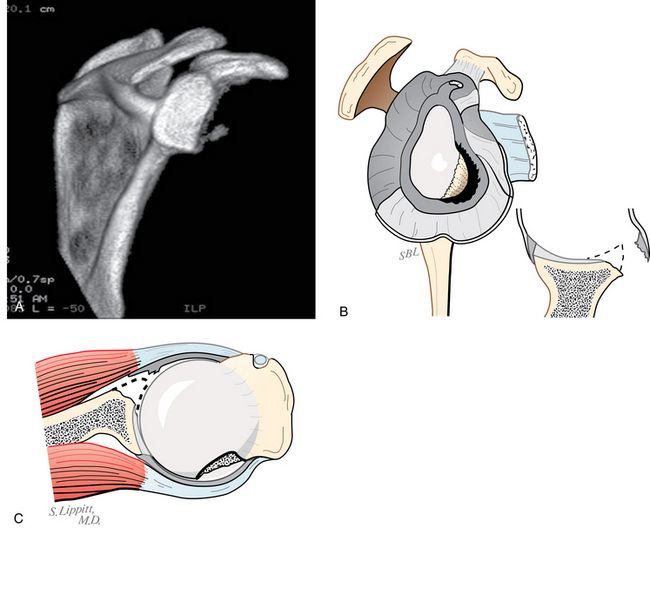
Plain radiographs and computer tomography (CT) are the recommended radiographic studies to document the direction of instability and evaluate osseous lesions. Anteroposterior views of the shoulder in internal and external rotation, an axillary lateral view, the Stryker notch view, and the Bernageau view will help diagnose most Hill-Sachs and glenoid fracture lesions. If an osseous lesion is suspected, a CT arthrogram and three-dimensional imaging of the glenoid are helpful in quantifying bone loss (Fig. 19-2). The CT arthrogram better defines the extent of bone loss when compared with an MR arthrogram of the shoulder. The dye in the CT arthrogram will outline the cartilaginous erosion and the three-dimensional reconstruction will allow assessment of bone loss according to Gerber et al.6 When evaluating the CT or MRI, the oblique sagittal reconstruction views provide the images necessary to calculate glenoid bone loss.
Description of technique for iliac crest autograft
Related posts:
 Pathology and findings in patients with multidirectional instability
Pathology and findings in patients with multidirectional instability
 Rehabilitation: return-to-play and in-season guidelines
Rehabilitation: return-to-play and in-season guidelines
 Radiographic studies and findings
Radiographic studies and findings
 Open treatment of multidirectional instability—surgical technique
Open treatment of multidirectional instability—surgical technique
 Humeral head defects—biomechanics, measurements, and treatments
Humeral head defects—biomechanics, measurements, and treatments
 Nonoperative rehabilitation for traumatic and atraumatic glenohumeral instability
Nonoperative rehabilitation for traumatic and atraumatic glenohumeral instability
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


