CHAPTER 126 On-the-field Assessment of the Cervical Spine-Injured Athlete
INTRODUCTION
Physicians caring for athletes during sports competition must be prepared to evaluate and treat injuries to the cervical spine. While most injuries are mild and self-limiting, injury to the spinal cord resulting in temporary or permanent neurologic injury is a rare but potentially catastrophic event. The medical team at sporting events must be prepared to assess, stabilize, and transport athletes with suspected cervical spine injuries.
Cervical spine trauma is most common in contact or collision sports such as American football, rugby, and ice hockey.1–6 Other sports such as gymnastics, skiing, wrestling, and diving also carry a higher risk of injury.1,7,8 American football has provided the largest population of athletes to follow with serious cervical spine injuries. The National Center for Catastrophic Sports Injury Research reported a total of 223 spinal cord injuries in American football between 1977 and 2001, with an incidence of cervical spinal cord injury in high school football of 0.52/100 000 participants, 1.55/100 000 participants in college football, and 14/100 000 participants in professional football.9 Cervical spinal cord injuries were also the most common catastrophic football injury and the second leading cause of death attributable to football.9
A NOTE ON ATHLETIC BRAIN INJURY AND CONCUSSION
Concussion is the most common sports-related head injury and is defined as a transient post-traumatic alteration in neural functioning. Concussive symptoms include confusion, dizziness, headache, visual disturbance, nausea, equilibrium disturbance, difficulty concentrating, post-traumatic amnesia, and loss of consciousness. Many classifications of concussion have attempted to grade the severity of concussion based on clinical presentation and duration of symptoms.10,11 Recent research involving neuropsychological testing pre- and post-concussion has better delineated which symptoms correlate with severity and the time needed for full recovery.12 Collins et al.12 showed that the presence of amnesia, not loss of consciousness, is the best predictor of concussion severity and neurocognitive deficits. For the sideline evaluation, no athlete with a concussion should be allowed to return to play if still symptomatic. Several references are available which summarize recent advances and recommendations in the management of athletic concussion.13–15
MECHANISM OF INJURY
Axial loading
The mechanism of injury to the cervical spine and associated anatomic risk factors that lead to serious neurologic injury have been the subject of active interest and debate within the sports medicine and spine surgery communities. Early research suggested that serious cervical spine injuries occurred from forced hyperflexion2–7,16 or hyperextension.17–20 However, more recently axial loading has been defined as the most likely mechanism for catastrophic injury to the cervical spine during sports competition.
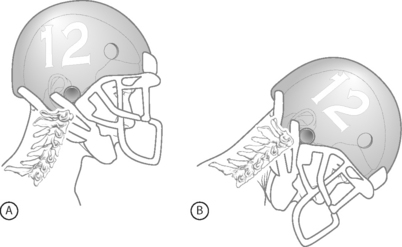
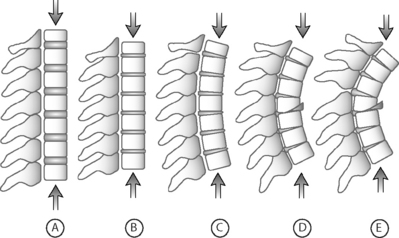
Axial loading occurs when a player strikes another player with the top of the head as the point of initial contact (so-called ‘spear tackling’). Axial loading places the cervical spine at a biomechanical disadvantage and makes it particularly susceptible to severe injury. Typically, most forces from a traumatic load to the cervical spine are dissipated through controlled spinal motion, the paravertebral muscles, and the intervertebral discs. When the top or crown of the helmet is used for initial contact, the neck is typically flexed approximately 30° and loses its normal cervical lordosis and ability to properly distribute force (Fig. 126.1). In this position the cervical spine assumes the characteristics of a segmented column and forces are transmitted along the longitudinal axis of the spine (Fig. 126.2).21
In athletes with cervical spinal stenosis, axial loading followed by forced hyperextension or hyperflexion can cause transient or permanent sensory and motor changes. Penning19 described a ‘pincer mechanism’ with compression of the spinal cord between a vertebral body and the spinolaminar line of an adjacent vertebra. Compression of the spinal cord occurs in hyperextension when the distance between the posteroinferior margin of the superior vertebral body and the anterosuperior aspect of the spinolaminar line of the subjacent vertebra decreases (Fig. 126.3). With hyperflexion, the anterosuperior aspect of the spinolaminar line of the superior vertebra and the posterosuperior margin of the inferior vertebra approximate. Eismont et al.20 also noted that hyperextension causes narrowing of the anteroposterior diameter of the spinal canal and can compress the spinal cord. Torg et al.22 described an axial load input with subsequent hyperextension and indentation of the ligamentum flavum with compression of the spinal cord. In each of these mechanisms, the anteroposterior diameter of the spinal canal decreases, resulting in compression of the spinal cord. Transient or permanent cervical cord injury can occur and usually involves a contusion of the spinal cord with temporary restriction of blood flow and a focal area of ischemia.8
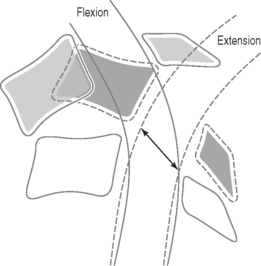
Fig. 126.3 Hyperextension ‘pincer mechanism’ as described by Penning.19 During hyperextension, the distance between the posteroinferior aspect of the superior vertebral body and the anterosuperior aspect of the spinal laminar line of the subjacent vertebra decreases, and the cord is pinched between the two vertebral bodies.
While advances in helmet materials and equipment used in American football lead to a decrease in head injuries, it also contributed to the development of dangerous playing techniques using the top of the helmet as the initial point of contact. Torg et al.23 compared the total number of head and neck injuries in the National Football League between 1971 and 1975 with previous work done by Schneider24 analyzing injuries between 1959 and 1963. The major difference between these time periods was the type and quality of helmet worn during competition. The study found a reduction in intracranial hemorrhages of 66% and deaths due to intracranial injury of 42%. However, the study also found a 204% increase in cervical spine fractures, subluxations, and dislocations and a 116% increase in the number of cases of permanent quadriplegia. The majority of cases of permanent quadriplegia that occurred were due to direct compression when a player struck another player with the top of his helmet.
Delineation of the axial load mechanism as the major cause of catastrophic cervical spine injury in American football resulted in rule changes that caused a sustained decrease in the rate of cervical spine injuries and quadriplegia. In 1976 the National Collegiate Athletic Association banned ‘spearing,’ defined as intentionally striking an opponent with the crown of the helmet, as well as other tackling techniques in which the helmet is used as the initial point of contact. In 1976, the rate of cervical spine fracture, subluxation, and dislocation was 7.72/100 000 and 30.66/100 000 in high school and college athletes, respectively. In 1987, this had decreased to 2.31/100 000 and 10.66/100 000 serious injuries to the cervical spine in high school and college athletes, respectively.21 Injuries resulting in permanent quadriplegia also significantly decreased as a result of the rule changes. In 1976, the rate of quadriplegia was 2.24/100 000 and 10.66/100 000 in high school and college athletes, respectively. In 1977, only 1 year after the rule changes, these rates decreased to 1.30/100 000 and 2.66/100 000 in high school and college athletes, respectively, and have continued to remain low.21
In 1990 Torg and colleagues25 further confirmed axial loading as the mechanism in catastrophic cervical spine injury by review of actual game films and videotapes. Analysis of films allowed an accurate determination of the mechanism of injury in 85% of cases, and axial loading was found to be the mechanism in every case.
INJURIES TO THE NECK AND SPINAL CORD
Stingers
‘Stingers’ or ‘burners’ are descriptive terms used to characterize transient unilateral upper extremity pain and paresthesias following a blow to the neck or shoulders. Because of confusion with a potentially more serious central cord injury called ‘burning hands syndrome,’26 use of the term ‘stinger’ rather than ‘burner’ is encouraged. Stingers are very common and are reported in up to 50–65% of college football players.27,28
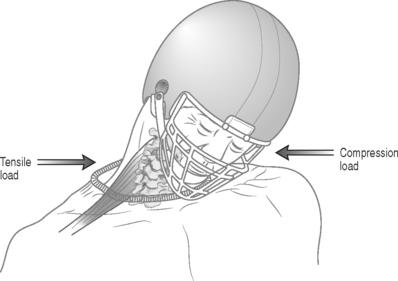
Stingers usually result from one of two mechanisms: tensile overload or compression overload.29 While either mechanism is possible in any athlete, the mechanism of injury is more likely depending on the age of the athlete. In most high school athletes, the mechanism involves a tensile or stretch injury when the involved arm and neck are stretched in opposite directions. This occurs as the neck is forcibly stretched away while the ipsilateral shoulder is depressed (Fig. 126.4). In the older college or professional athlete with a higher likelihood of degenerative changes of the cervical spine, a compressive mechanism is more likely. This involves a compression or ‘pinch’ of the cervical nerve root within the neural foramen as the neck is forcibly flexed in a posterolateral direction towards the symptomatic upper extremity (see Fig. 126.4).30
Recurrent stingers are more common in the presence of cervical degenerative disc disease. Levitz et al.30 studied 55 athletes with recurrent stingers. The mechanism of injury was extension combined with ipsilateral compression in 83% of patients, and 70% had a positive Spurling’s sign. Eighty-seven percent of patients had evidence of disc disease by magnetic resonance imagimg (MRI), and 93% had disc disease or narrowing of the intervertebral foramina. The authors concluded that nerve root compression in the intervertebral foramina secondary to degenerative disc disease was the likely cause of recurrent or chronic stinger syndromes in collegiate and professional athletes. Athletes with more than one stinger can be placed in a protective neck collar that limits lateral neck flexion and hyperextension.
Rarely, more significant nerve injury and axonotmesis occurs causing chronic symptoms. Patients usually demonstrate persistent weakness in the distribution of the upper trunk of the brachial plexus, and muscle atrophy may be present in severe cases. Electromyography will assess the distribution and degree of injury and should be performed if symptoms have lasted more than 3 weeks. Most cases of axonotmesis have a high likelihood of recovering within 1 year.27
Cervical cord neurapraxia and transient quadriplegia
Injury to the spinal cord can be complete or be neurapraxic – a reversible injury with motor and sensory function returning within 24–48 hours. Neurapraxia of the cervical spinal cord is characterized by an acute, transient sensory and/or motor change to more than one extremity. Symptoms include burning pain, numbness, tingling and loss of sensation with or without motor changes of paresis or complete paralysis.31 Several other terms have been used to describe cervical cord neurapraxia and have been used interchangeably, including ‘transient quadriplegia,’31 ‘central cervical spinal cord syndrome,’32 and ‘spinal cord concussion.’33
The most typical pattern of incomplete spinal cord injury is the central cord syndrome. This involves weakness of the upper extremities in excess of lower extremity findings secondary to the lamination of the corticospinal tracts and selective damage to fibers serving arm and hand function. ‘Burning hands syndrome’ described by Maroon26 is characterized by burning dysesthesias of the hands and associated weakness of the upper extremities and is a variant of central cord syndrome. Transient quadriplegia is a temporary paralysis characterized by loss of motor function, with or without sensory disturbances.31
Episodes of cervical cord neurapraxia are transient by definition and complete recovery usually occurs in 10–15 minutes, although in some patients gradual resolution occurs over 1–2 days. Except for burning paresthesia, the athlete does not experience neck pain, and there is complete return of motor function and full, pain-free range of motion of the cervical spine. Torg et al.34 studied 110 patients with transient cervical cord neurapraxia and found that 40% presented with plegia (complete motor weakness), 25% with paresis (incomplete motor weakness), and 35% with only paresthesia and sensory symptoms. The neurapraxia resolved in 74% of patients within 15 minutes and lasted more than 24 hours in 11% of patients. Eighty percent of patients had symptoms in all 4 extremities, 15% in the upper extremities only, 2% in lower extremities only, and 3% with symptoms in the ipsilateral upper and lower extremities. Of 110 patients, 109 had a complete neurologic recovery, with one patient having a residual hemiplegia following operative intervention. For those athletes who did return to football, the recurrence rate for transient cervical cord neurapraxia was 56% with no athlete experiencing permanent neurologic injury, although the follow-up period was only 3 years and some athletes chose to retire from collision sports.
Cervical spinal stenosis
The method to best determine spinal stenosis in an athlete has been the subject of considerable debate. Early definitions used the absolute anteroposterior canal diameter to detect spinal stenosis – measured from the posterior aspect of the vertebral body to the most anterior point on the spinolaminar line. In general, a canal was considered normal if the diameter between C3 and C7 was >15 mm, and spinal stenosis was present if the diameter was <12 mm.35
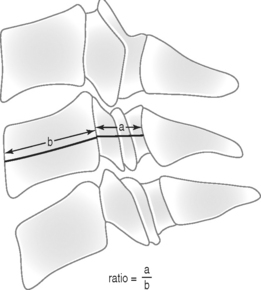
Torg et al.31 and Pavlov et al.36 described a measurement to detect spinal stenosis using a spinal canal to vertebral body ratio (known as the ‘Torg ratio’). The ratio uses the anteroposterior diameter of the spinal canal and the anteroposterior width of the midpoint of the vertebral body (Fig. 126.5). The measurements are made at the level of the third through the sixth vertebral body on a routine lateral radiograph of the cervical spine. The ratio method eliminates error caused by magnification factors or differences in target-to-film distances. A spinal canal-vertebral body ratio of <0.8 indicates significant spinal stenosis. In Torg’s study,31 a ratio of <0.8 was recorded at one or more levels in 24 athletes with cervical cord neurapraxia, compared to a ratio of 1.0 or more in 49 age-matched controls with no neurologic complaints.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


