Obstructive Sleep Apnea Syndrome
Carole L. Marcus
Obstructive sleep apnea syndrome (OSAS) is an important cause of morbidity in children. If left untreated, it can result in cor pulmonale, neurologic impairment, and failure to thrive. Pediatric OSAS was rediscovered when it was described in detail by Christian Guilleminault and colleagues in 1976. However, descriptions of this syndrome date back to the writings of William Osler, more than a century ago.
Obstructive apnea is defined as the cessation of airflow at the nose and mouth, despite continued respiratory effort, secondary to upper airway obstruction. This is distinct from central apnea, in which cessation of airflow is associated with absent respiratory effort. Many children with OSAS exhibit continuous partial airway obstruction, associated with hypoxemia and hypoventilation, rather than complete airway obstruction; this has been termed obstructive hypoventilation.
EPIDEMIOLOGY
The prevalence of OSAS in the pediatric age group is estimated to be 2% of preschool children, as reported by Redline and colleagues. The peak incidence is between approximately 2 to 6 years of age. However, OSAS can occur at any age, from the neonatal period through adolescence. In prepubertal children, in contrast to adults, OSAS occurs equally among boys and girls.
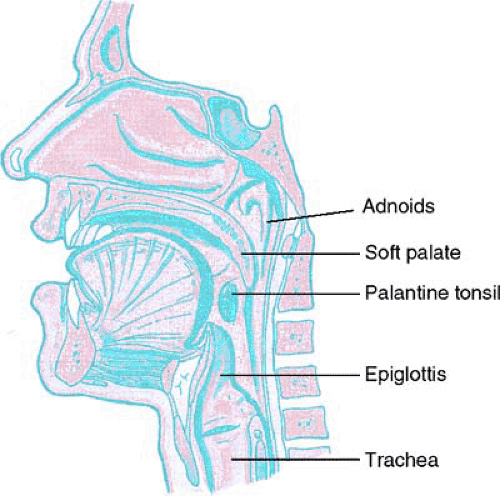 FIGURE 238.1. Diagram of the upper airway. (Reprinted from Moore KL, Augur AMR. Essential clinical anatomy, 2nd ed. Baltimore: Lippincott Williams & Wilkins, 2002.) |
PATHOLOGY
The upper airway above the level of the epiglottis (i.e., the nasopharynx, oropharynx and hypopharynx) is a hollow, neuromuscular tube (Fig. 238.1). It is usually patent, but it has the potential to collapse to facilitate speech and swallowing. In patients with OSAS, the upper airway collapses abnormally during sleep.
OSAS results from a combination of abnormal neuromuscular control and anatomic narrowing of the upper airway. During wakefulness, the patient with a narrow airway can compensate by augmenting upper airway muscle tone; thus, OSAS does not occur. During sleep, there is a decrease in ventilatory drive and in neuromuscular tone that facilitates upper airway collapse. In contrast, patients with obstruction in the cartilaginous portion of the upper airway have fixed obstruction during both wakefulness and sleep. This is associated with stridor rather than snoring.
In children, the anatomic narrowing of the upper airway is usually the result of adenotonsillar hypertrophy. Other common causes of structural narrowing include craniofacial anomalies and obesity. Patients with neuromuscular disorders resulting in hypotonia (e.g., muscular dystrophy) or incoordination of the upper airway musculature (e.g., cerebral palsy) are also at increased risk for OSAS. Children with syndromes encompassing developmental delay, hypotonia, obesity, and upper airway narrowing (e.g., children with trisomy 21) are at very high risk for OSAS (Box 238.1).
CLINICAL MANIFESTATIONS AND COMPLICATIONS
Most children present with a history of snoring and difficulty with breathing during sleep. The onset is usually insidious. Children with OSAS have persistent, loud snoring that can often be heard outside the bedroom. During sleep, the child has labored breathing, retractions, and paradoxical inward motion of the chest wall during inspiration. During periods of complete obstruction, the child can be observed to be making respiratory efforts, but no snoring is heard and no airflow is detected. Obstructive episodes are usually terminated by gasping, movements, or arousal from sleep. The child sleeps restlessly and may adopt unusual sleeping positions, such as sleeping in a seated position or with the neck hyperextended. Diaphoresis, pallor, or cyanosis may be present. The appearance of the child during sleep can be so alarming that it is not unusual for parents to maintain bedside vigils or to stimulate or reposition the child continually throughout the night. Nevertheless, many parents do not volunteer a history of their child’s sleep symptoms unless specifically asked. In the clinic, it is useful to ask parents to mimic their child’s snoring and breathing pattern.
BOX 238.1. Conditions Commonly Associated with Obstructive Sleep Apnea Syndrome*
Primarily Structural
Adenotonsillar hypertrophy
ObesityRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



