Modified Dunn Procedure for Slipped Capital Femoral Epiphysis
Wudbhav N. Sankar
DEFINITION
The modified Dunn procedure is an open realignment of the capital femoral epiphysis performed through a surgical dislocation approach.18
Like the original Dunn osteotomy, the modified Dunn corrects a slipped capital femoral epiphysis (SCFE) at the site of maximal deformity (ie, the physis).4
The procedure can be performed on both unstable SCFEs and stable SCFEs.
ANATOMY
The main source of perfusion to the femoral epiphysis is the medial femoral circumflex artery (MFCA) (FIG 1).
The deep branch of the MFCA runs posterior to the obturator externus and perforates the hip capsule just distal to the piriformis and proximal to the superior gemellus.5
It ends in two to four retinacular branches that enter the superior aspect of the femoral head.
The intact external rotator muscles, especially the obturator externus, protect the MFCA during surgical dislocation of the hip.
To safely reduce a SCFE, which typically displaces posterior and inferior to the neck, tension must be minimized on the retinacular vessels.18
PATHOGENESIS
The pathogenesis of a SCFE is well discussed in Chapter 111.
The posteroinferior translation of the epiphysis relative to the femoral neck alters the resting position of the femoral head within the acetabulum.
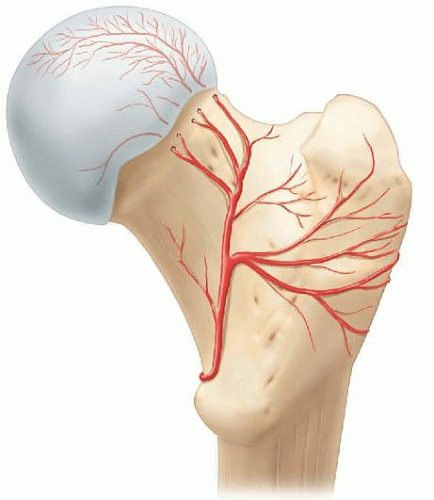
FIG 1 • Posterior view of the vascular anatomy of the proximal femur. Note the proximity of the terminal branches of the MFCA to the insertion of the piriformis tendon.
This altered position combined with the residual offset of the metaphysis can dramatically affect the motion of the hip joint.
With flexion and internal rotation, the metaphyseal prominence can either enter the joint potentially causing damage to the acetabular cartilage or abut against the acetabular rim and the labrum13 (FIG 2).
In situ fixation, while effective for preventing further slippage, does not correct the deformity associated with SCFE.
NATURAL HISTORY
Historically, the long-term outcome after in situ screw fixation has generally been considered to be good.1, 2
Recent studies, however, have established an association between the residual proximal femoral metaphyseal deformity left by in situ treatment and the development of femoroacetabular impingement, lost hip motion, and premature osteoarthritis.6, 9, 11, 17
Increasing slip severity has been associated with poorer outcome.3
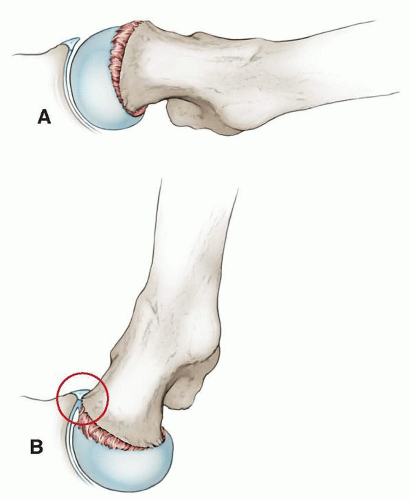
FIG 2 • Clinical implication of a residual SCFE deformity: With flexion and internal rotation, the metaphyseal prominence can either enter the joint potentially causing damage to the acetabular cartilage (A) or abut against the acetabular rim and the labrum (B).
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients with an unstable SCFE usually present acutely with an abrupt onset of symptoms.
Pain is intense and can be elicited even with simple logrolling of the affected extremity.
By definition, patients with unstable SCFE are unable to ambulate with or without walking aids.10
Further forced range of motion (ROM) of the affected hip is discouraged to minimize the risk of additional trauma to the femoral head blood supply.
Patients with severe, stable SCFE can present with variable duration of symptoms.
Patients complain of hip or groin pain, thigh pain, or knee pain and usually occurs without a history of trauma.
By definition, patients are able to ambulate with or without walking aids and typically present with an antalgic gait and an external foot progression angle.10
Hip flexion, abduction, and internal rotation in the flexed position will be markedly decreased in a severe SCFE as a result of femoroacetabular impingement.
Many patients will also demonstrate obligate external rotation which is forced external rotation that results from passive hip flexion.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Plain radiographs of the pelvis, including anteroposterior (AP) and frog-leg lateral views, should be obtained in any pediatric patient with hip, thigh, or knee pain and are generally diagnostic of a SCFE.
The femoral epiphysis is typically displaced posterior (on the frog view) and slightly inferior (on the AP view) in relation to the femoral neck.
A widened physis on AP or lateral views can be an early sign of SCFE.
The severity of a SCFE can be described by displacement relative to the width of the metaphysis:
Mild: less than one-third the width
Moderate: one-third to half the width
Severe: more than half the width
Another method of describing slip severity is measuring the difference between the epiphyseal shaft angle on each side16:
Mild: less than 30 degrees
Moderate: 30 to 50 degrees
Severe: 50 degrees or greater
In cases with delayed presentation in which the modified Dunn is being considered, computed tomography (CT) scan can be used to more accurately assess the degree of displacement and the amount of physeal closure.
In certain patients with unstable SCFEs who present late, bone scan or contrast magnetic resonance imaging (MRI) can be used to assess the perfusion to the epiphysis.
DIFFERENTIAL DIAGNOSIS
SCFE
Legg-Calvé-Perthes disease
Hip labral tear
Femoral neck fracture
Septic arthritis of the hip
Knee derangement
Greater trochanteric bursitis
NONOPERATIVE MANAGEMENT
Immobilization in a spica cast was the historical treatment but is no longer recommended for SCFE.
Once SCFE is identified in any patient with an open physis, management is surgical to avoid further slippage and the possible development of femoral head avascular necrosis (AVN).
SURGICAL MANAGEMENT
The modified Dunn procedure is indicated for unstable SCFEs and for certain stable SCFEs in which the residual deformity that would be left by in situ fixation is deemed unacceptable.
It is most easily performed when the physis is still open.
The modified Dunn procedure is a technically demanding procedure that requires familiarity with the surgical dislocation approach and the development of the retinacular flap.
Alternative techniques for treating unstable SCFEs include (1) positional reduction followed by percutaneous screw fixation (with at least two screws) and capsular decompression7 or (2) gentle manual open reduction performed via an anterolateral approach followed by Kirschner wire (K-wire) or screw fixation.12
Alternative techniques for treating severe stable SCFEs include in situ fixation followed by osteoplasty of the femoral head-neck junction and/or proximal femoral osteotomy.
Preoperative Planning
All imaging studies are reviewed.
Both AP and frog views should be reviewed for the presence of posteroinferior callus. This finding implies some chronicity to the SCFE and its removal is necessary to achieve an anatomic reduction.
Pure displacement (ie, angulation or translation) can be corrected via the modified Dunn, but some chronic changes such as femoral neck retroversion are more difficult to address.
In chronic and severe stable SCFEs, CT scans can be used to assess the status of the physis and determine the indication for the modified Dunn procedure.
The contralateral hip should be evaluated both clinically and radiographically to determine whether a SCFE is present.
In younger patients, and those with endocrinopathies, prophylactic percutaneous screw fixation of the normal side should be considered. This can be done in the supine position before commencing with the modified Dunn procedure (see Chap. 111).
Timing of surgery for an unstable SCFE is somewhat controversial. For cases that present overnight, the author prefers performing the modified Dunn procedure the next morning with an appropriately skilled surgical team.
Positioning
As with a standard surgical dislocation of the hip (see Chap. 109), the patient is placed in full lateral position, secured on a pegboard. A flat-top cushion (with cutout for the down leg) supports the operative extremity during the procedure (FIG 3).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








