Metal on Polyethylene
Arun Kannan
William A. Jiranek
In total hip arthroplasty (THA), metal femoral heads articulating with polyethylene liners has stood the test of time and remains the most commonly used bearing couple in hip arthroplasty (1,2). The introduction of cross-linked polyethylene has been the most significant advance in bearing technology for THA in the last two decades. While cross-linked polyethylene has decreased clinical wear and improved the survival of THA, it is not without trade-offs and has necessitated changes in acetabular component design. In this chapter, we focus on rarer complications such as liner fractures, liner dissociations, and trunnion damage, directly or indirectly attributable to metal-on-polyethylene articulations.
Case Example
A 65-year-old man presented with a 1-week history of squeaking in his replaced right hip following an episode of popping felt while playing golf, 4 years after his primary THA. The radiographs obtained at 3 months after the primary THA (Fig. 90.1A) and after the onset of symptoms are shown in Figure 90.1. Figure 90.1B shows eccentric positioning of the head and articulation against the metallic acetabular shell, consistent with liner dissociation. One must look for clues in the operative report and pre-event radiographs for possible cause of dissociation.
The liner was found dissociated at surgery. There was no evidence of liner fracture, but the effect of impingement of the femoral neck on the liner was apparent (Fig. 90.2, region between arrows), with blunting of the inner edge of the liner. The pre-event radiographs had been consistent with acetabular retroversion.
Liner Dissociation
Locking Mechanism and Acetabular Design
The locking mechanism between the modular acetabular component and the polyethylene liner has evolved continuously over the last two decades. The first-generation modular
acetabular components employed a variety of locking mechanisms. The Harris-Galante (HG) cup introduced in the 1980s had four pairs of titanium prongs (also referred to as tines) along the rim that locked into slots in the circumference of the liner. The porous-coated anatomic (PCA) cup had a circumferential flange on the liner that locked into a corresponding slot in the cup. The first-generation cups had a relatively high rate of failure secondary to liner dissociation that was attributable to the liner locking mechanism (3,4,5,6). The so-called second-generation acetabular components commonly employed a locking ring in the acetabular component. The Duraloc cup (DePuy, Inc., Warsaw, Indiana), for example, had a locking ring with multiple bends that expanded on insertion of the liner and locked into a slot on the liner. The second-generation components employing the locking rings had a much higher push-out and lever-out strength as compared to the first-generation components (7). The second-generation cups involved lateralization of the head with thinner polyethylene at the rim than at the dome. The lateralized head was covered at the equator by a thin rim of liner not supported by the metal cup (8). The advent of cross-linked polyethylene led to further changes in cup design. The inferior resistance to fracture of the cross-linked polyethylene led manufacturers away from unsupported polyethylene. The majority of the current generation of acetabular components have therefore given up the locking ring mechanism. The locking mechanism employed by the major manufacturers is listed in Table 90.1. Most manufacturers use a taper or interference fit between the cup and the liner recessed in the interior of the cup, away from the rim and, in addition, have antirotation tabs or scallops in varying numbers to resist torsional forces. The lever-out and push-out strength of some third-generation cups are lower than that of the second-generation cups.
acetabular components employed a variety of locking mechanisms. The Harris-Galante (HG) cup introduced in the 1980s had four pairs of titanium prongs (also referred to as tines) along the rim that locked into slots in the circumference of the liner. The porous-coated anatomic (PCA) cup had a circumferential flange on the liner that locked into a corresponding slot in the cup. The first-generation cups had a relatively high rate of failure secondary to liner dissociation that was attributable to the liner locking mechanism (3,4,5,6). The so-called second-generation acetabular components commonly employed a locking ring in the acetabular component. The Duraloc cup (DePuy, Inc., Warsaw, Indiana), for example, had a locking ring with multiple bends that expanded on insertion of the liner and locked into a slot on the liner. The second-generation components employing the locking rings had a much higher push-out and lever-out strength as compared to the first-generation components (7). The second-generation cups involved lateralization of the head with thinner polyethylene at the rim than at the dome. The lateralized head was covered at the equator by a thin rim of liner not supported by the metal cup (8). The advent of cross-linked polyethylene led to further changes in cup design. The inferior resistance to fracture of the cross-linked polyethylene led manufacturers away from unsupported polyethylene. The majority of the current generation of acetabular components have therefore given up the locking ring mechanism. The locking mechanism employed by the major manufacturers is listed in Table 90.1. Most manufacturers use a taper or interference fit between the cup and the liner recessed in the interior of the cup, away from the rim and, in addition, have antirotation tabs or scallops in varying numbers to resist torsional forces. The lever-out and push-out strength of some third-generation cups are lower than that of the second-generation cups.
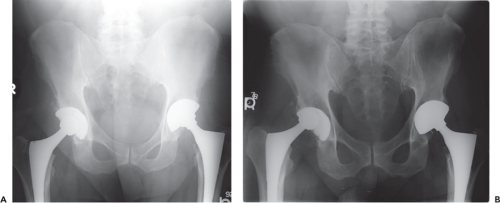 Figure 90.1. A 65-year-old man presented with a 1-week history of squeaking in his replaced right hip following an episode of popping felt while playing golf, 4 years after his primary THA. The radiographs obtained at 3 months after the primary THA (A) and after the onset of symptoms are shown above. B: It shows eccentric positioning of the head and articulation against the metallic acetabular shell, consistent with liner dissociation. |
 Figure 90.2. The patient demonstrated in Figure 90.1 was taken up for surgery and the liner was found to be dissociated from the acetabular cup. There was no evidence of liner fracture, but the effect of impingement of the femoral neck on the liner was apparent (region between blue arrows), with blunting of the inner edge of the liner. The pre-event radiographs had been consistent with acetabular retroversion. |
Liner Dissociation: Clinical Reports
The first-generation HG cups were known to have a high rate of failure secondary to failure of the peculiar locking mechanism. The breakage of the tines in the HG cup led to dissociation and revisions for these involved a revision of the acetabular component or cementing of a liner into a well-fixed acetabular component (5,9). The second-generation acetabular components with locking rings probably had the strongest locking mechanism and have given way to the third-generation components designed to accommodate cross-linked polyethylene liners. There have been several case reports of acute liner dissociations from the third-generation acetabular components (Table 90.2) (10,11,12). Mesko et al. reported that a review of the MAUDE-FDA database revealed 25 cases of liner dissociation involving a third-generation component between December 2006
and January 2008 (10). It is however not possible to estimate the incidence as the denominator remains unknown. It also remains to be seen if the failure is specific to one specific manufacturer or is a class effect common to third-generation acetabular components that do not employ a locking ring. It also merits mention in this context that locking tabs are made of cross-linked polyethylene which has inferior ultimate tensile strength and may be more susceptible to failure than the conventional polyethylene.
and January 2008 (10). It is however not possible to estimate the incidence as the denominator remains unknown. It also remains to be seen if the failure is specific to one specific manufacturer or is a class effect common to third-generation acetabular components that do not employ a locking ring. It also merits mention in this context that locking tabs are made of cross-linked polyethylene which has inferior ultimate tensile strength and may be more susceptible to failure than the conventional polyethylene.
Table 90.1 Locking Mechanism in Current Generation Acetabular Components | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||
Table 90.2 Case Reports of Liner Dissociation with Modern Cementless Cups | |||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Risk Factors for Liner Dissociation
Factors that lead to failure of the locking mechanism are well studied with the HG cups. The surgical and patient factors (other than those related to the design of the locking mechanism itself) are probably common to HG cups and the current generation acetabular components. Easily avoidable surgical factors include incomplete seating of the liner, residual debris between the cup and the liner, or a combination of the two resulting in eccentric loading of the liner giving rise to a lever-out force. Most manufacturers suggest visual and tactile confirmation of the complete seating of the locking tabs; none of the designs have a more objective method of confirming this.
Impingement is a known factor that places excessive stress on the locking mechanism (5,13). Intra-articular impingement directly causes edge loading of liner and a contrecoup force that drives the hip toward subluxation. Although extra-articular impingement does not have edge loading at the site of impingement, it still produces the contrecoup force diametrically opposite to the site of impingement and eccentrically loads the articulation. The importance of the activities that a patient with a THA indulges in should not be underestimated. A patient who consistently indulges in activities that border on the range to impingement may cause recurrent eccentric loading of even well aligned components. Most case reports on dissociation of liners in current generation acetabular components have not had component orientation beyond the safe range.
Management of Liner Dissociation
Patients with liner dissociations often present with recent onset of symptoms. A patient reporting a sudden clunk followed by squeaking should arouse the suspicion for a dissociated liner. Radiographs would reveal eccentric positioning of the head, with the femoral head directly against the metal-backed acetabular component. While the treatment of these patients should be conducted in an expeditious manner to prevent damage occurring from the unintended articulation between the femoral head and the metal backing of the cup, the standard workup for a revision hip arthroplasty including a complete set of radiographs and infection evaluation must be carried out before embarking on a revision. Radiographs to ascertain implant fixation, component orientation, and condition of the locking rings and bone stock would help one anticipate problems that might occur at surgery. Replacement liners may not be available for acetabular components or the exact sizes may not be available. The importance of tracing
the implant details from the primary surgery cannot be overemphasized.
the implant details from the primary surgery cannot be overemphasized.
At surgery, one may find black or dark gray staining of tissues consistent with metallosis. Cell count and differential count of the hip aspirate obtained intraoperatively along with intraop frozen sections would be valuable, especially if the preoperative workup was equivocal. The retrieved liner should be labeled to define orientation, and should be examined for evidence of wear, impingement, and damage to the locking mechanism. The cup should be closely scrutinized for the integrity of the locking mechanism. A reassessment of cup and stem orientation may reveal the etiology of dissociation. Impingement should be ruled out by placing a trial liner and if present, be classified as intra-articular or extra-articular.
When the cup is well fixed and well positioned with an intact locking mechanism, we would replace with a modular neutral liner. If the cup is placed in excessive abduction or abnormal version with evidence of intra-articular impingement, it should be reoriented irrespective of the status of the locking mechanism. If the acetabular component is well positioned, but with a compromise of the locking mechanism, the options are to either revise the acetabular shell, or cement a polyethylene liner into a well-fixed shell.
Several authors have reported excellent success with cementation of a polyethylene liner into a well-fixed acetabular component (14,15,16,17,18) and this has been backed by biomechanical analysis (19). A cement mantle of 2 to 4 mm has been suggested as the minimum required for performing this technique (18). This type of reconstruction is particularly useful in patient with poor bone stock, difficult acetabular reconstructions, or poor medical condition as it avoids the difficulties encountered with acetabular explantation and reconstruction. Yoon et al. (15




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
