Malunions of the Proximal
T. F. Ritzman: Department of Orthopaedic Surgery, Clinic Lerner School of Medicine, Cleveland, Ohio.
J. P. Iannotti: Department of Orthopaedic Surgery, Cleveland Clinic Foundation, Cleveland, Ohio.
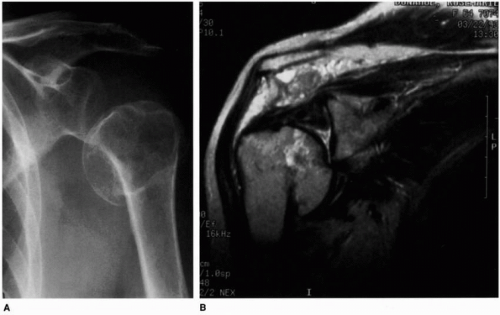 Figure 17-1 (A) Anatomic neck malunion in a 64-year-old woman with an associated axillary nerve injury and deltoid paralysis. (B) Magnetic resonance (MR) scan demonstrates a posttraumatic arthritis defect in the humeral head, early avascular necrosis, and marked deltoid and supraspinatus atrophy. In this case, the MR scan is helpful in diagnosing the avascular necrosis, determining the degree of atrophy and detecting posttraumatic arthritis. |
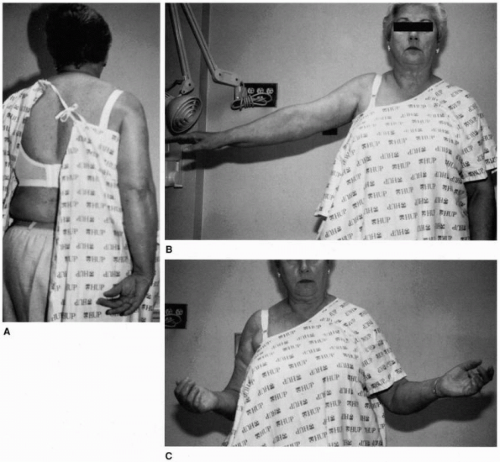 Figure 17-2 (A) The patient’s functional disability from the marked loss of internal rotation, (B) abduction, and (C) external rotation, primarily resulting from capsular contracture, necessitating open capsular release. |
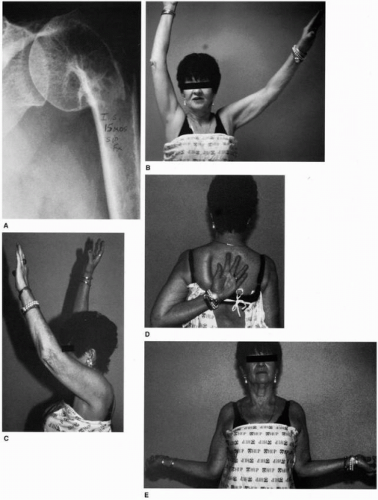 Figure 17-3 (A) A 60-year-old woman had a humeral neck malunion after prior surgery. The patient had excellent function in (B) abduction, (C) forward flexion, (D) internal rotation, and (E) external rotation. |
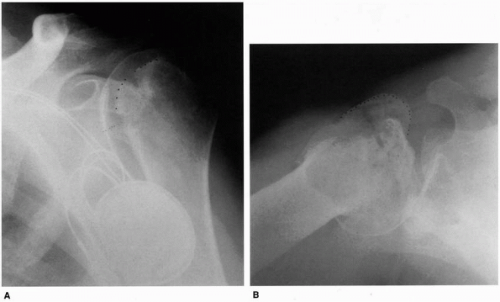 Figure 17-4 A 60-year-old retired but active man sustained a fall that produced pain. (A) An anteroposterior and inadequate scapular Y-view did not demonstrate the posterior humeral head dislocation. Malunion of a lesser tuberosity fracture with a posterior dislocation was initially unrecognized because of the lack of an axillary view at the time of the initial injury. (B) The axillary view obtained 6 months after injury clearly demonstrates posterior subluxation, malunited tuberosities, and posttraumatic arthritis. The dotted line represents the greater tuberosity. |
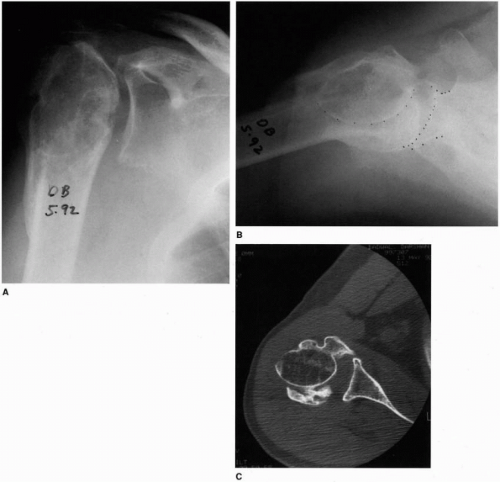 Figure 17-5 A 45-year-old businessman sustained a fall in India that was treated with nonoperative care. He had only mild pain with the activities of daily living and therefore did not consent to surgery. This patient had only 70 degrees of elevation and 0 degrees of external rotation and internal rotation to the buttock. (A) Malunion of a four-part fracture is poorly defined on the anteroposterior view. (B) The axillary view improves the recognition of the displaced humeral head fragment (widely spaced dotted line), and (C) the CT scan best defines the united tuberosities.
Related posts: Three-Part Fractures: Open Reduction and Internal Fixation, or Arthroplasty?
Anterior Superior Rotator Cuff Tears: Repairable and Irreparable Tears
Massive Tears of the Posterosuperior Rotator Cuff
Special Issues in Inflammatory Arthritis
The Failed Arthroplasty: Options for Revision
Arthrodesis and Other Salvage Procedures: When Arthroplasty Is Not Indicated Three-Part Fractures: Open Reduction and Internal Fixation, or Arthroplasty?
Anterior Superior Rotator Cuff Tears: Repairable and Irreparable Tears
Massive Tears of the Posterosuperior Rotator Cuff
Special Issues in Inflammatory Arthritis
The Failed Arthroplasty: Options for Revision
Arthrodesis and Other Salvage Procedures: When Arthroplasty Is Not Indicated
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|