Magnetic Resonance Imaging in the Upper Extremity
Courtney T. Tripp
John F. Feller
The opinions and assertions expressed herein are those of the authors and should not be construed as reflecting those of the Department of Defense.
SHOULDER
High sensitivity and specificity for diagnosis of both labral and rotator cuff abnormalities have been demonstrated with magnetic resonance imaging (MRI) on 1.5-T scanners, with even greater sensitivity and specificity demonstrated recently with higher strength 3.0-T scanners (10,14,15,39). Although some authors advocate the routine use of magnetic resonance arthrography (MRA) for evaluation of the labrum and partial-thickness rotator cuff tears (37), the increasing availability of 3.0-T MRI may obviate the need to perform MRA in the future.
Traumatic shoulder dislocation/subluxation is a common athletic injury, and MRI can provide valuable information regarding the integrity of the capsulolabral, cartilaginous, and osseous structures, which may be injured.
The normal glenoid labrum on MRI is a uniformly hypointense ovoid rim of fibrocartilage at the margin of the glenoid and is triangular in shape on cross-sectional imaging. The joint capsule, along with multiple band-like regions of capsular thickening known as glenohumeral ligaments, attaches directly to the glenoid labrum.
The most common injury associated with traumatic shoulder dislocation is a Bankart lesion, a detachment of the anteroinferior labrum and capsule from the glenoid rim, first described by Bankart in 1923 (2) (Fig. 46.1). A number of “Bankart variants” have subsequently been described, all of which involve injury of the anteroinferior capsulolabral complex and are associated with clinical shoulder instability (19) (Fig. 46.2). A tear (detachment) of the glenoid labrum is diagnosed on MRI as abnormal morphology of the labrum and/or curvilinear hyperintensity traversing the labrum or between the base of the labrum and glenoid rim.
A Hill-Sachs lesion is an osseous impaction injury of the posterolateral humeral head, which is often seen on MRI subsequent to anterior shoulder dislocation (Fig. 46.3). An osseous avulsion of the anteroinferior glenoid, which is important to surgical management, can also be seen and is known as a “bony Bankart” lesion.
Superior labral tear from anterior to posterior (SLAP) lesions of the glenoid labrum are common injuries in athletes and represent tears of the superior labrum that extend in an anterior to posterior direction (Fig. 46.4). Four types of SLAP lesions were originally described by Snyder and colleagues and have been demonstrated to be accurately diagnosed on high-resolution noncontrast MRI (10,23) and MRA (16,35):
Type 1 lesions are characterized by degenerative fraying of the free edge of the superior labrum.
Type 2 tears are unstable lesions with avulsion of the superior labrum and biceps anchor from the glenoid.
Type 3 lesions constitute a bucket handle tear of the superior labrum with an intact biceps anchor.
Type 4 lesions constitute a bucket handle tear of the superior labrum with extension into the biceps anchor (30).
The classification of SLAP lesions has been expanded further into several additional types, which principally represent combinations of the most common form, SLAP type 2 lesion, with other associated injuries of the labrum and capsular structures (18). However, the original Snyder classification remains the most widely used (37).
Tendinosis of the proximal long head of the biceps tendon occurs frequently in association with impingement syndrome and rotator cuff tears (usually subscapularis or leading edge of supraspinatus). Biceps instability, manifest on MRI with medial subluxation/dislocation of the biceps tendon at the level of the intertubercular groove, is associated with injury to the structures of the rotator interval (coracohumeral ligament, superior glenohumeral ligament, superior subscapularis tendon, and anterior supraspinatus tendon) (21).
Impingement syndrome (IS) of the shoulder is a clinical diagnosis and constitutes a range of pathology affecting the rotator cuff beginning with mild tendinosis and progressing to partial- and full-thickness rotator cuff tear (RCT) and finally rotator cuff arthropathy.
Although IS is a clinical syndrome, MRI can provide supportive diagnostic confidence by revealing any number of findings that are highly associated with IS, including a type
III acromion process, a subacromial enthesophyte, tendinosis and/or partial- or full-thickness tears of the rotator cuff, rotator cuff muscle atrophy with fatty infiltration, and subacromial subdeltoid bursal fluid.
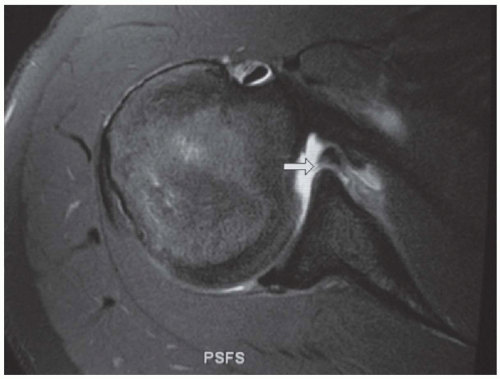
Figure 46.1: Axial fat suppression intermediate-weighted MRI demonstrating evidence of prior unidirectional anterior instability with a torn anterior labrum (Bankart lesion) (arrow).
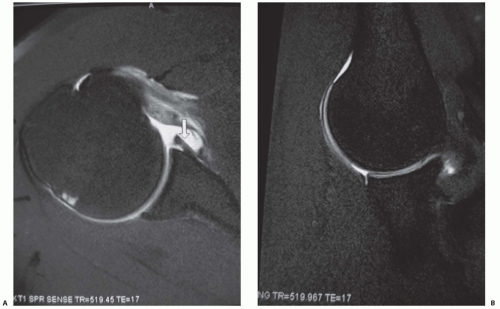
Figure 46.2: A: Axial fat suppression intermediate-weighted MRI of the shoulder demonstrating an anterior labral tear, a Bankart variant lesion (Perthes lesion) with an intact scapular periosteum (arrow). B: Abduction-external rotation (ABER) fat suppression intermediate-weighted MRI of the same shoulder further demonstrating the Bankart variant lesion (Perthes lesion) with an intact scapular periosteum (arrow).
Normal tendons appear as uniformly hypointense curvilinear bands on all MRI sequences.
Tendinosis is seen as either abnormal morphology and/or abnormal hyperintense signal of a tendon, but not fluid-like signal intensity; findings are true for all tendons imaged on MRI.
Tendon tears demonstrate abnormal morphology and hyperintense fluid-like signal intensity of the tendon with partial or complete focal tendinous discontinuity. MRI has been demonstrated to be highly accurate for diagnosis of rotator cuff tendon tears (91% sensitivity and 88% specificity for all tears in a study conducted by Zlatkin et al. [39], and 95% and 84% accurate for full- and partial-thickness tears, respectively, in a study by Raffii et al. [26]). Fluid distention of the subacromial subdeltoid bursa is a secondary sign often seen associated with RCT.

Figure 46.3: Coronal T1 MRI of the same shoulder demonstrating a Hill-Sachs deformity of the posterosuperior humeral head; further evidence of prior unidirectional anterior instability.
In the case of full-thickness RCT, the degree of tendon retraction and muscle atrophy/fatty infiltration should be noted because these findings portend poorer postsurgical functional outcomes and can significantly influence clinical management (8,36). On MRI, muscle atrophy is diagnosed as fatty infiltration of the muscle (linear/streaky T1 hyperintense signal throughout the muscle) and decreased overall muscle bulk.
The use of abduction-external rotation (ABER) positioning sequences in shoulder MRI can aid in detection of intraarticular pathology. Tirman et al. (32) found increased detection rates of partial-thickness articular surface RCTs with imaging in the ABER position on MRA in overhead-throwing athletes, and Cvitanic et al. (7) found increased accuracy in detection of anteroinferior labral injuries with imaging in the ABER position.
Internal posterosuperior impingement (PSI) of the shoulder occurs commonly in overhead movement (throwing, tennis) athletes when the posterior glenoid labrum and rotator cuff tendons (supraspinatus and infraspinatus) are repeatedly wedged between the humeral head and posterosuperior glenoid rim during maximal cocking of the arm in abduction and external rotation. MRI findings of PSI include partial articular-sided tearing of the supraspinatus and infraspinatus tendons, posterosuperior labral abnormalities and glenoid degenerative changes, and cystic changes in the superolateral humeral head (6) (Fig. 46.5).
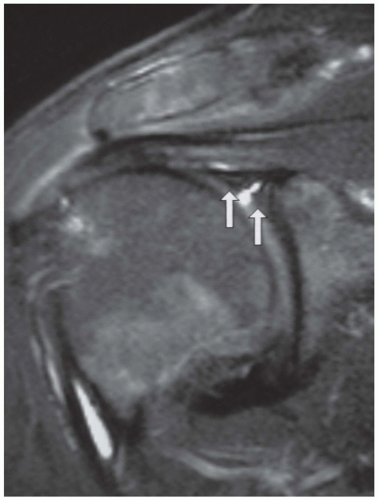
Figure 46.4: Coronal fat suppression intermediate-weighted MRI demonstrating a superior labral anterior to posterior (SLAP) type 2 lesion of the superior labrum. Arrows denote torn and separated portions of the labrum, with intervening bright fluid signal seen.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree






