Chapter Six Test items, test criteria, and associated impairments
Lower and Upper Quarter Movement Impairment Examinations
Introduction
Movement Impairments: Lower Quarter Examination
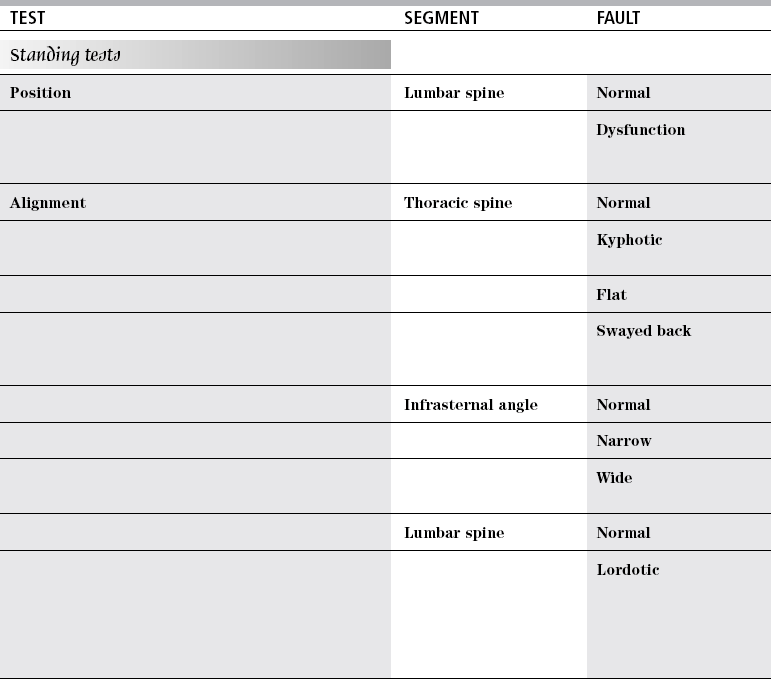
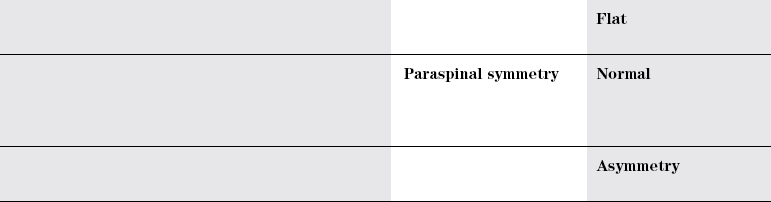
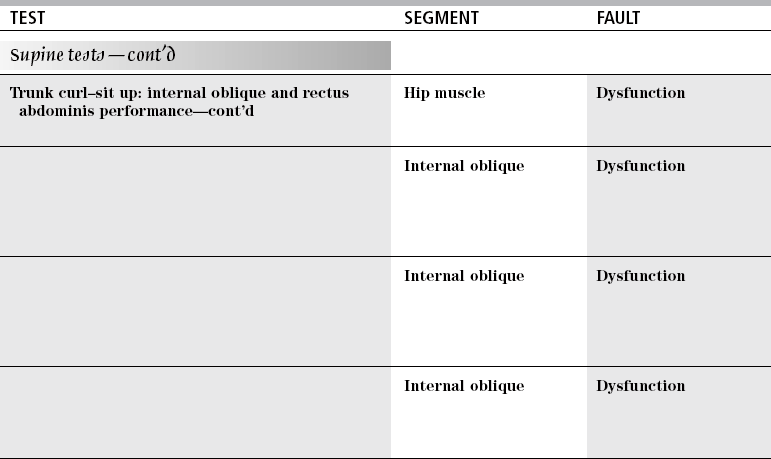
TEST
SEGMENT
FAULT
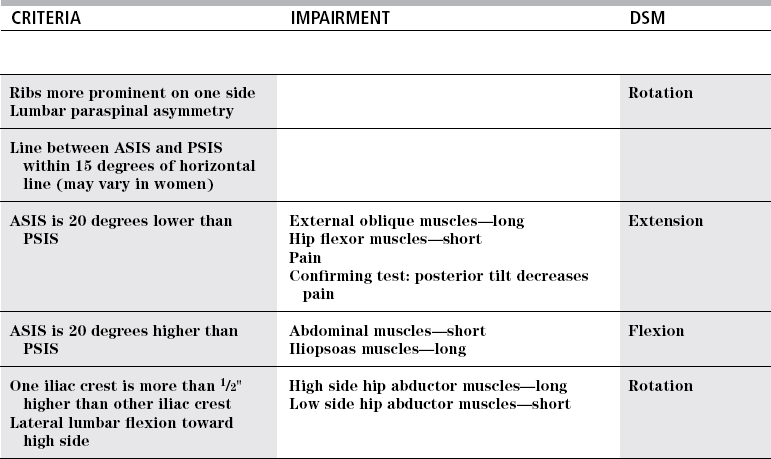
Scoliosis
Rib hump
Pelvis
Normal
Anterior tilt
Posterior tilt
Lateral tilt
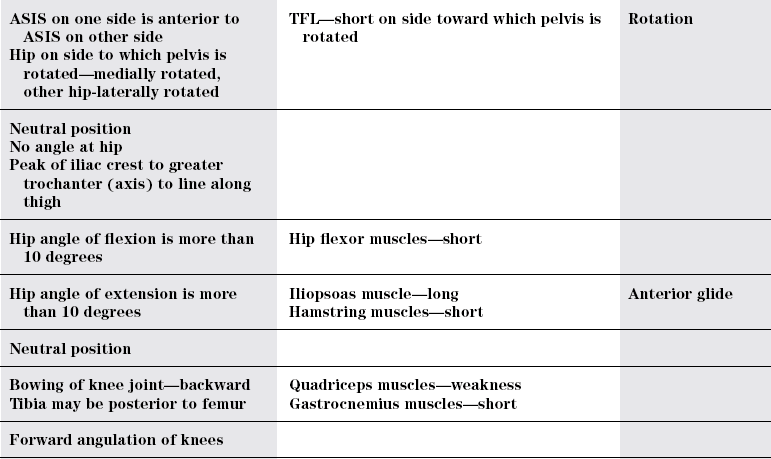
Rotation
Hip joint
Normal
Flexed
Extended
Knees
Normal
Hyperextended
Flexed
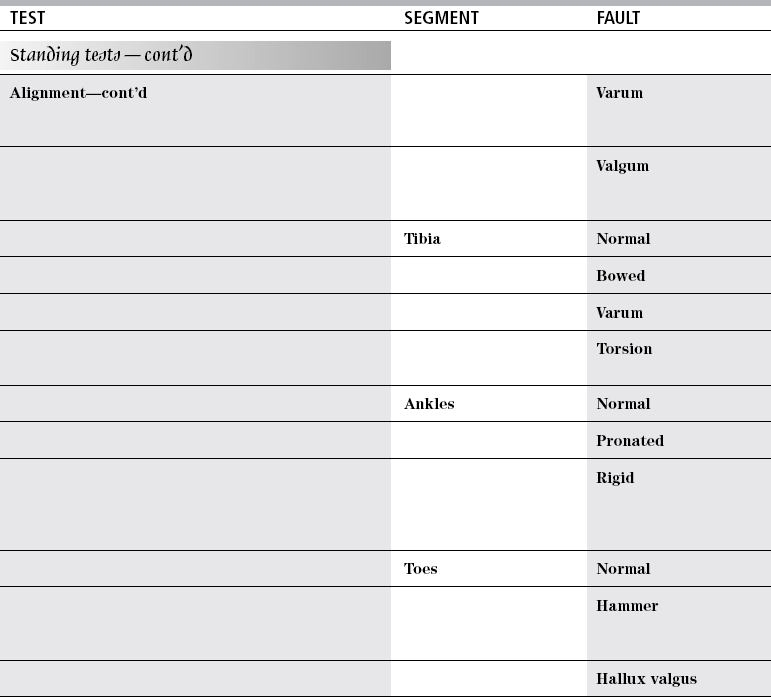
TEST
SEGMENT
FAULT
Lateral rotation
Ankle
Longitudinal arch
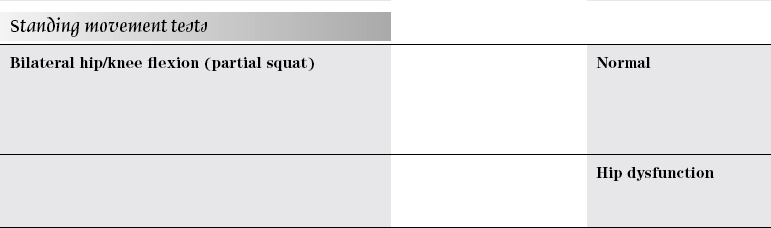
Single leg stance
Normal
Other hip flexed to 70 degrees
Lateral trunk flexion
Hip adduction
Pelvic rotation
Hip rotation
Forward bending
Normal
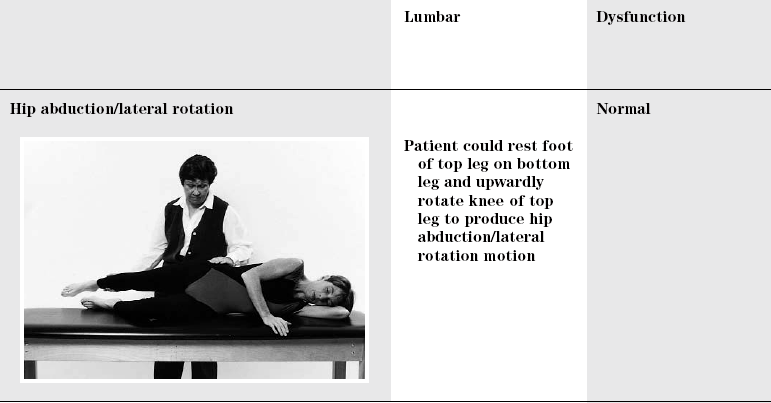
Lumbar
Dysfunction
TEST
SEGMENT
FAULT
Hip dysfunction
Ankle dysfunction
Return from forward bending
Normal
Lumbar dysfunction
Hip sway
Side bending
Normal
Lumbar dysfunction
Lumbar dysfunction
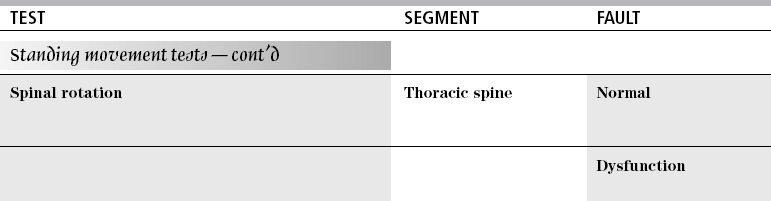
TEST
SEGMENT
FAULT
Lumbopelvic dysfunction
Hip muscle
Dysfunction
Hip joint
Dysfunction
Knee joint
Dysfunction
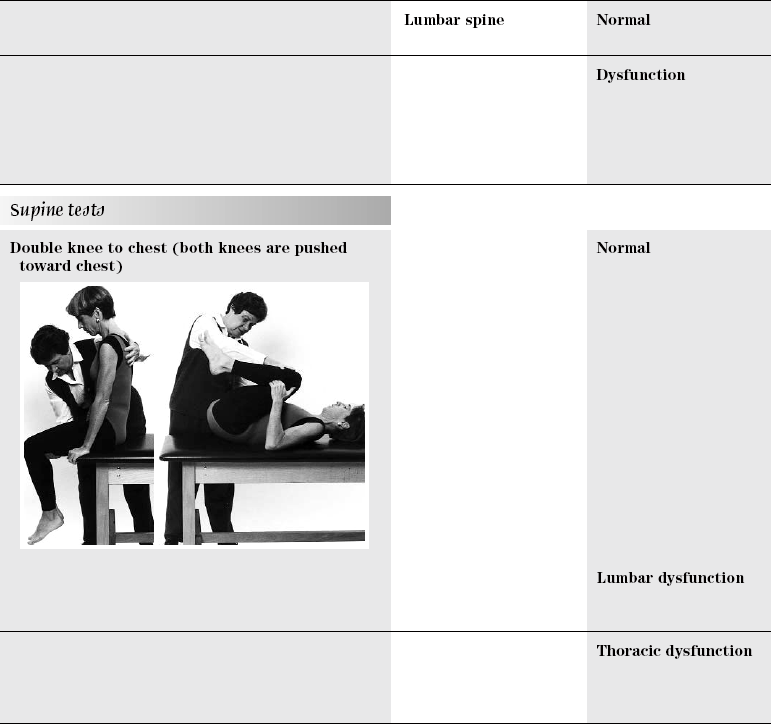
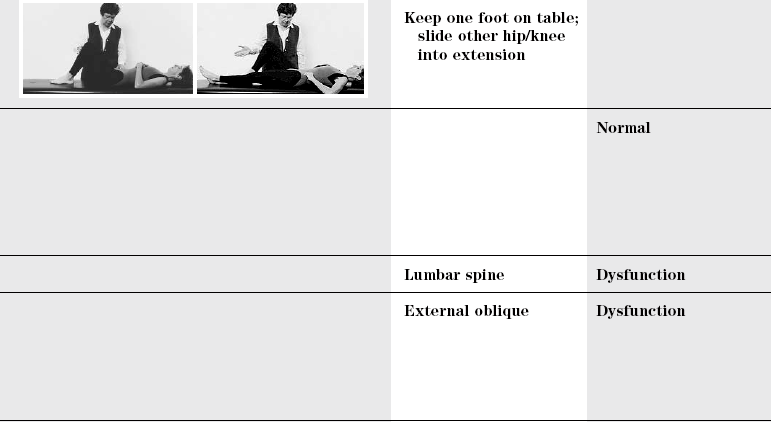
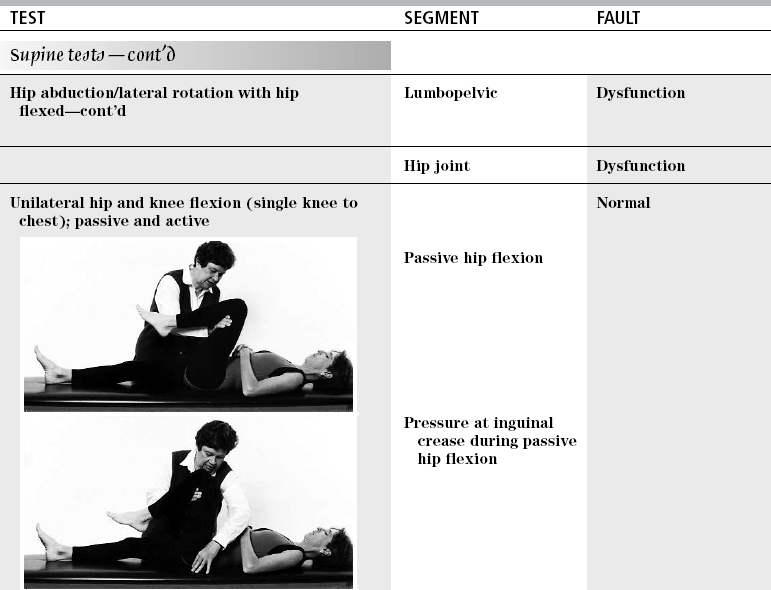
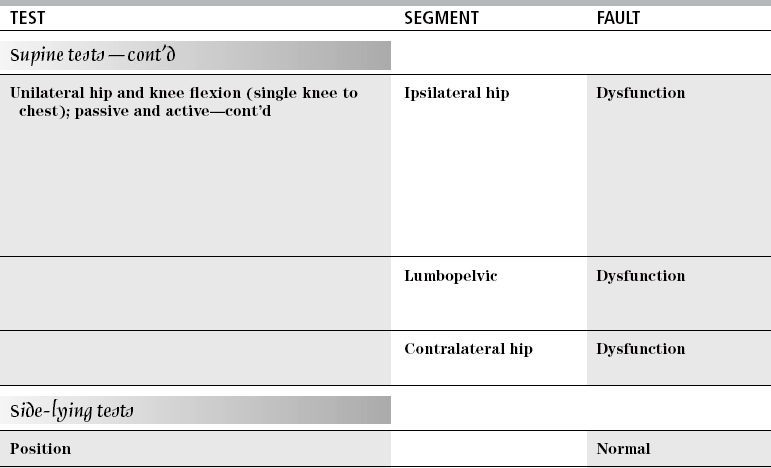
Supine position
Normal
Lumbar
Dysfunction
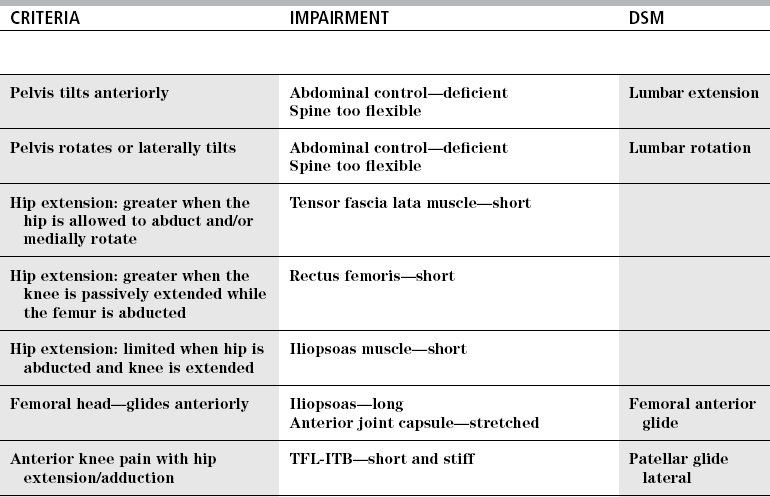
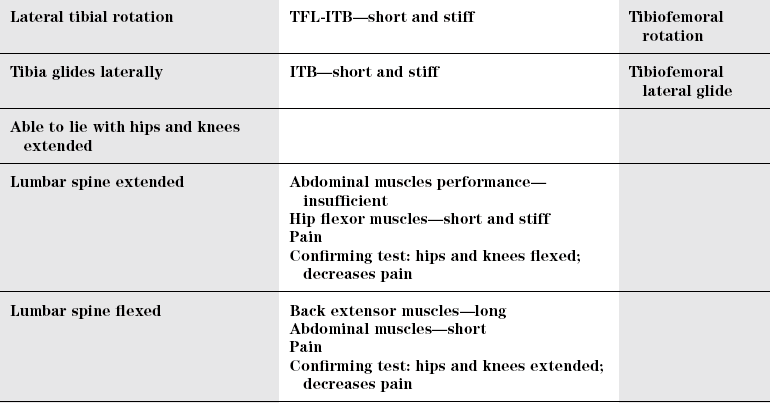
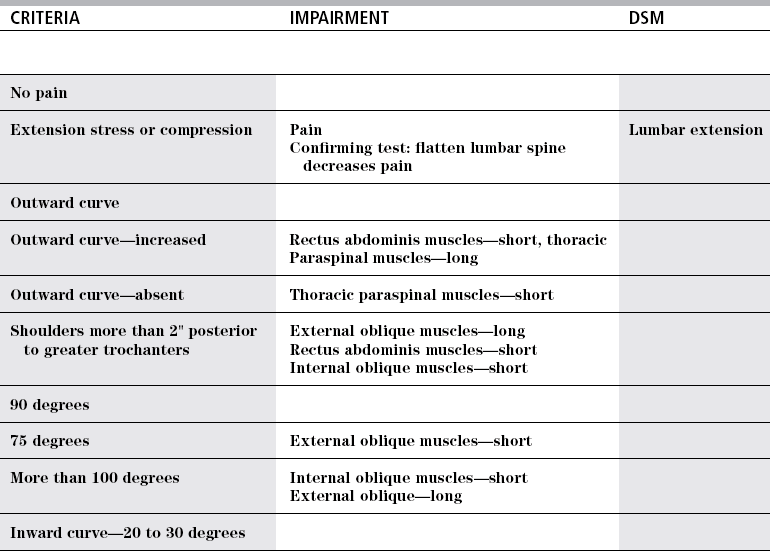
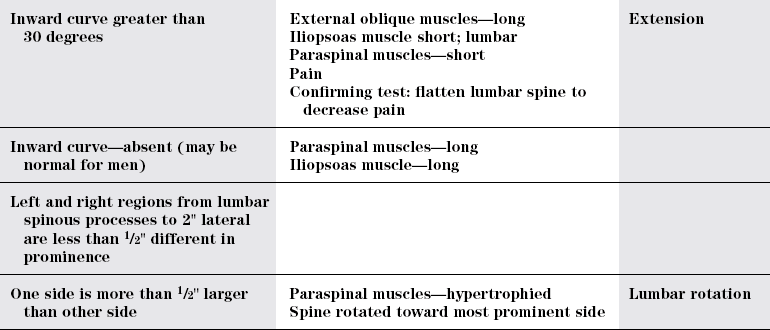
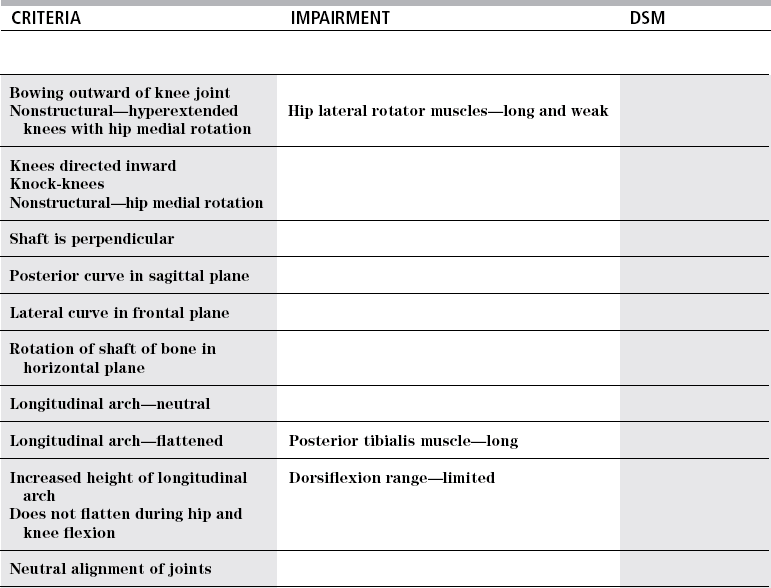
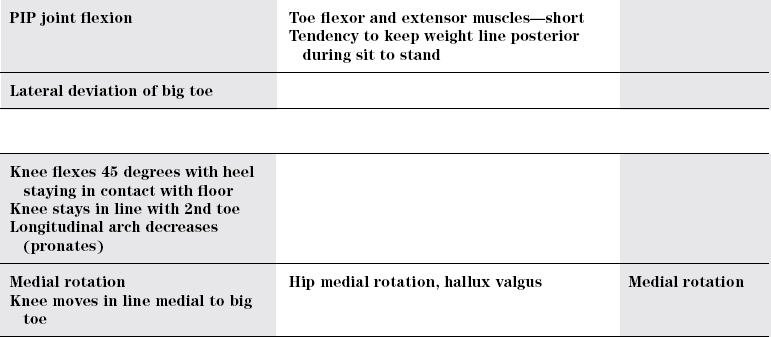
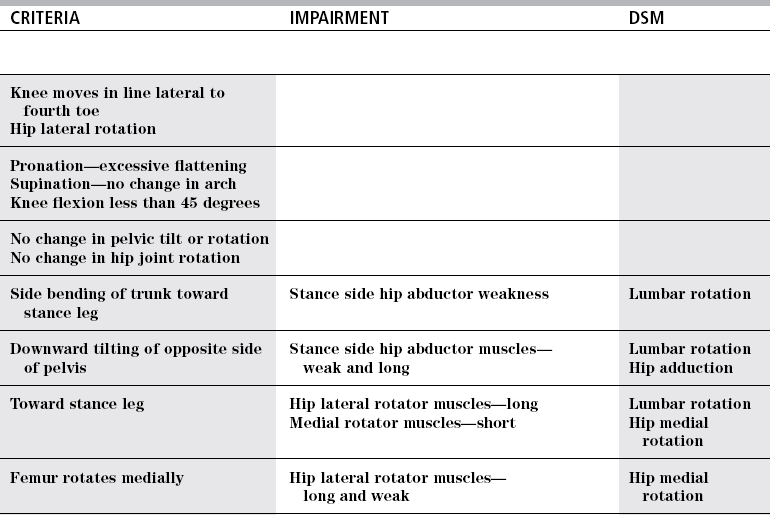
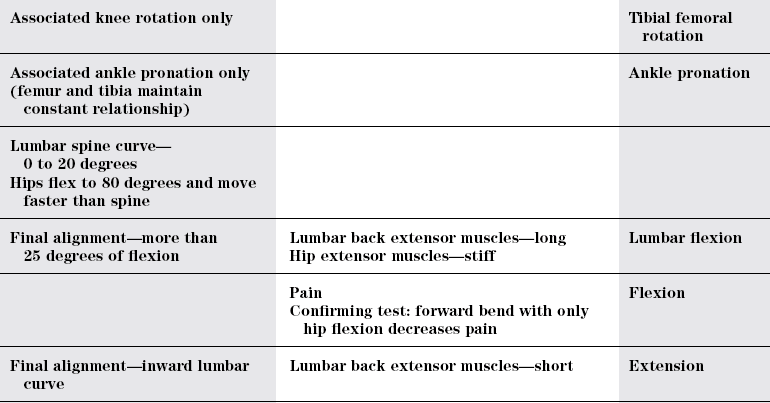
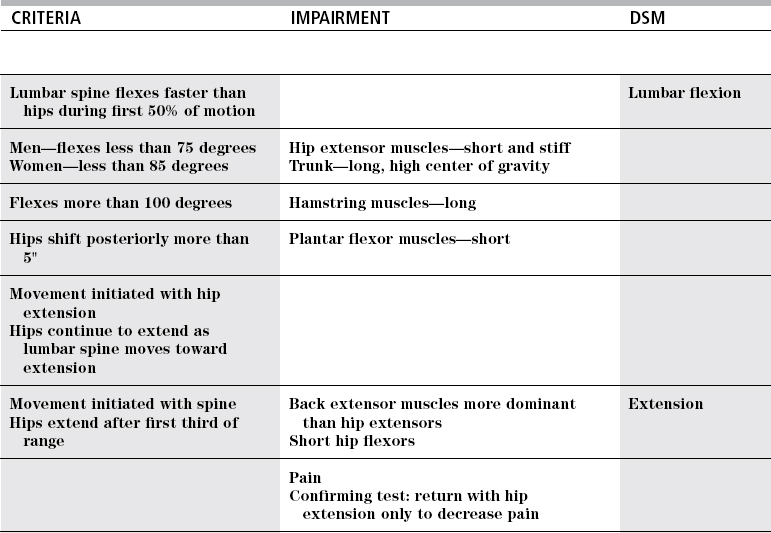
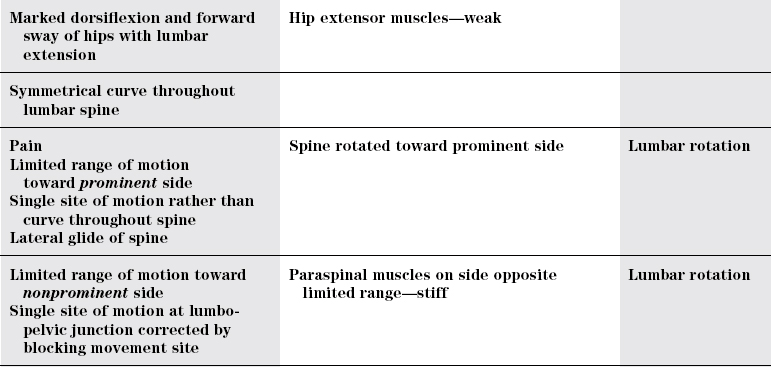
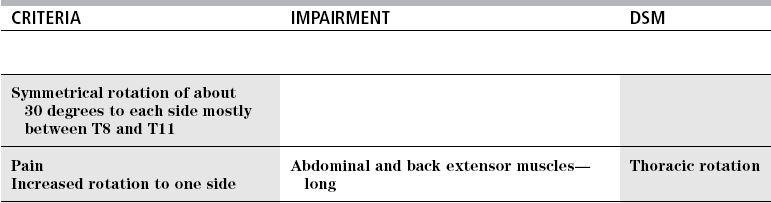
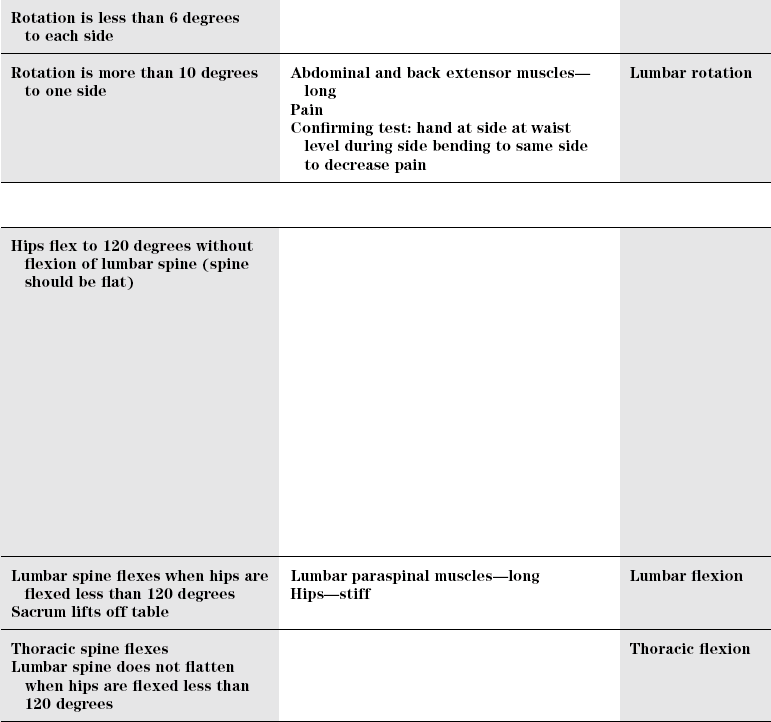
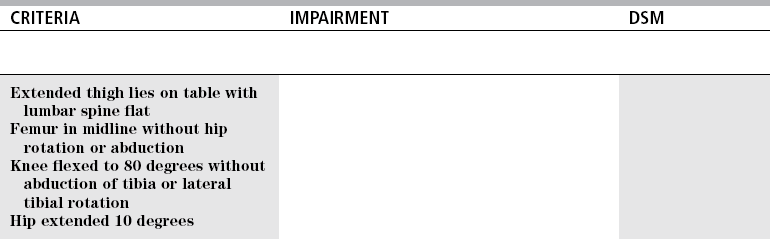
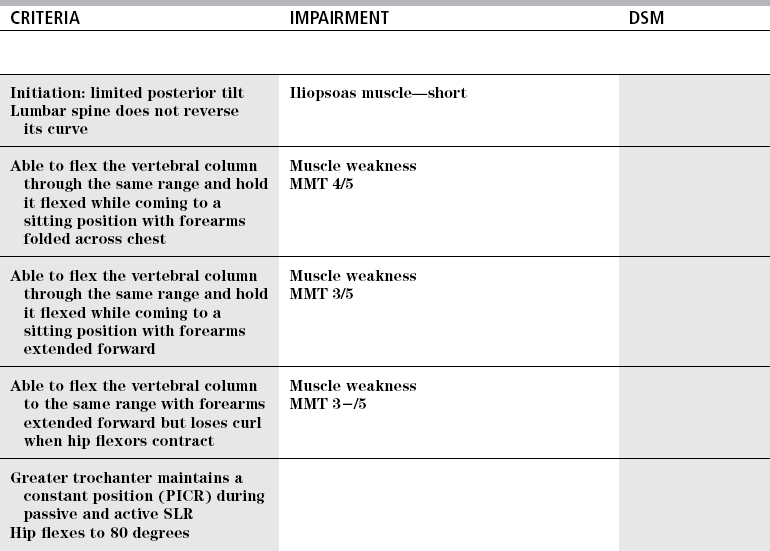
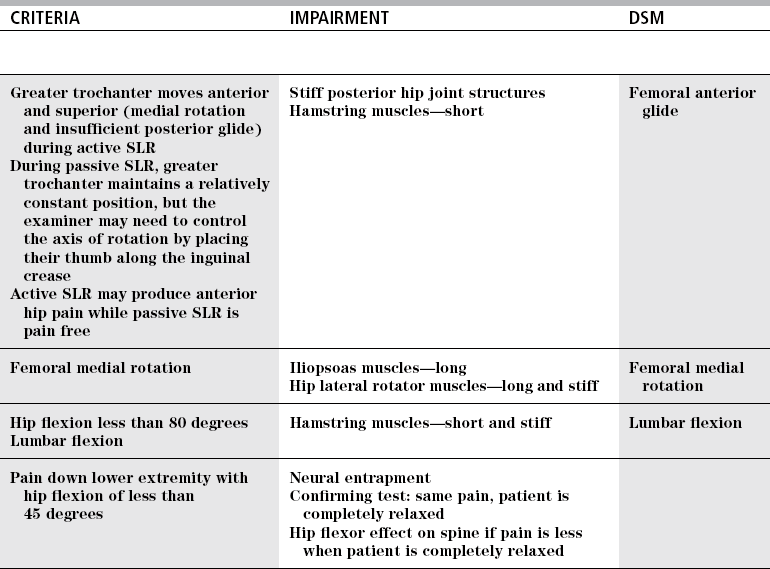
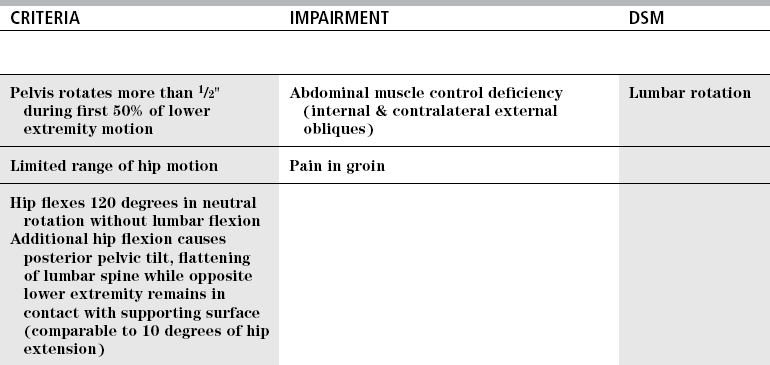
CRITERIA
IMPAIRMENT
DSM
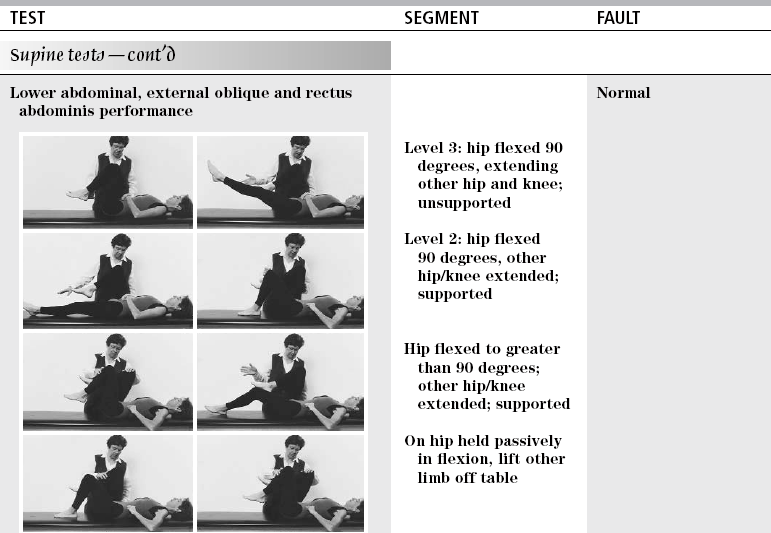
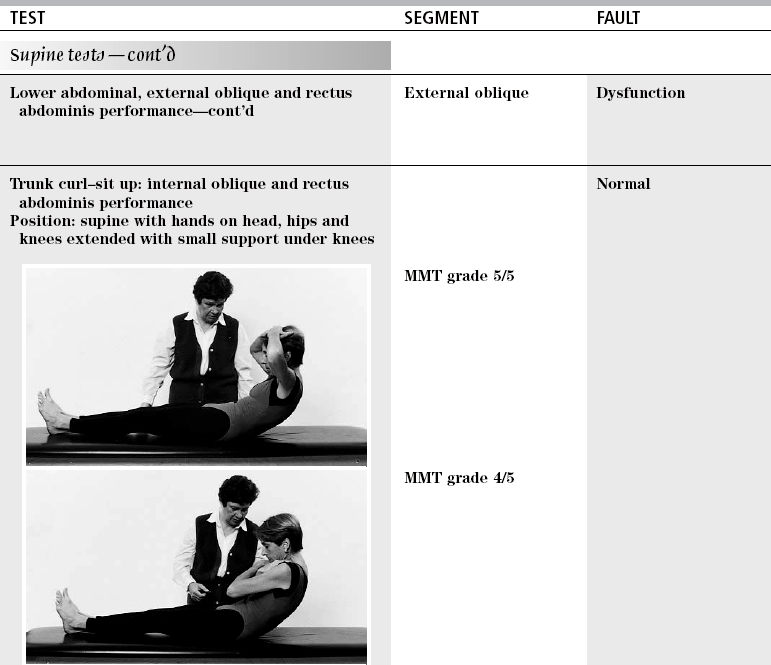
Maximal performance: double-leg lowering, while maintaining flat lumbar spine and posterior pelvic tilt
MMT grade 5/5
Minimal performance: maintain one hip at 90 degrees of flexion, back flat, while other lower extremity is extended and lowered to supporting surface while maintaining lumbar spine flat and pelvis in posterior pelvic tilt
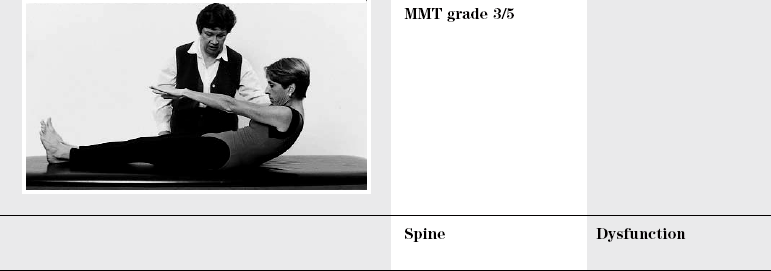
MMT grade 3/5
Anterior shear on lumbar spine
Pain with hip flexion
One hip flexed to 90 degrees while other lower extremity is extended while lightly touching heel to supporting surface and able to maintain lumbar spine flat and pelvis in posterior tilt
MMT grade 2/5
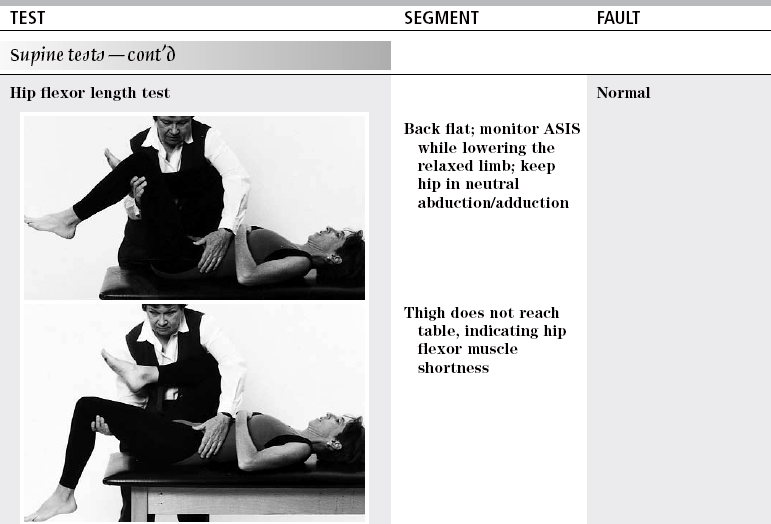
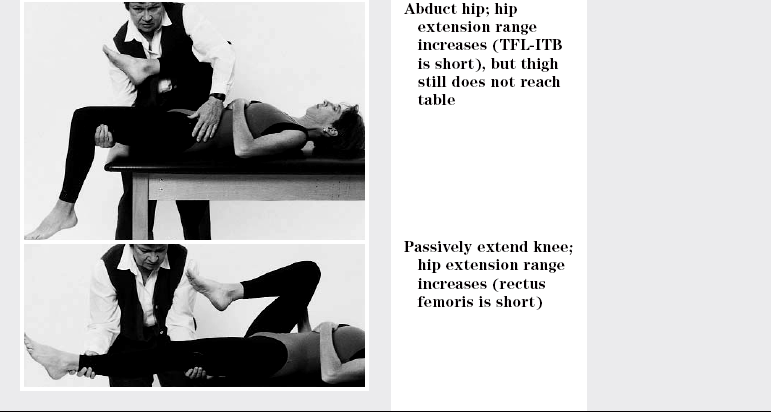
TEST
SEGMENT
FAULT
Hip
Dysfunction
Lumbar
Neural dysfunction
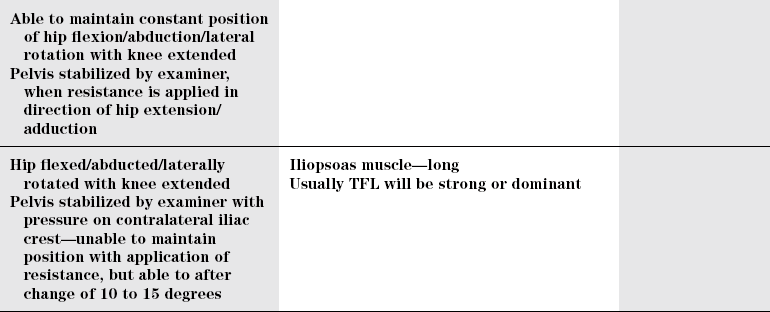
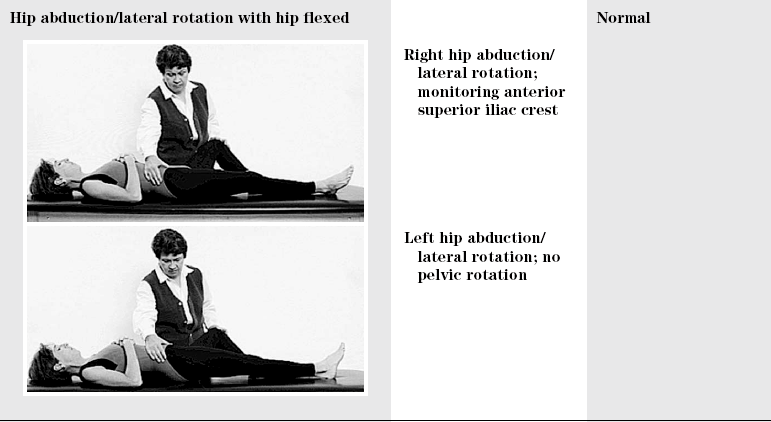
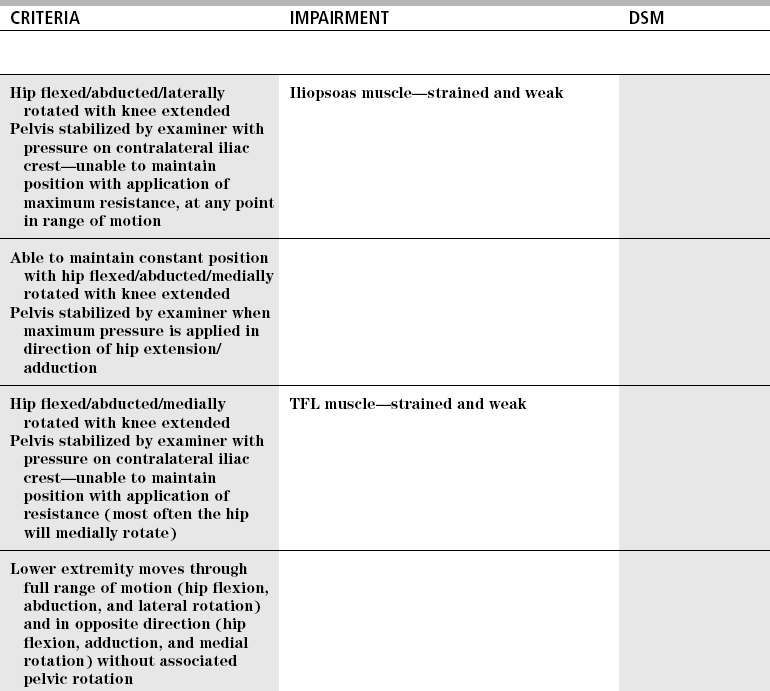
Iliopsoas
Muscle performance
Normal
Hip muscle
Dysfunction
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Lower and Upper Quarter Movement Impairment Examinations