Chapter 12. Injuries to the upper limb
Brachial plexus lesions
Brachial plexus lesions are serious and tragic. The most frequent victims are young men thrown from their motorcycles who may become unemployable as a result of their injuries.
Closed injuries
Closed injuries can occur in two ways:
1. By violent lateral flexion of the neck with depression of the shoulder or forced abduction of the arm.
2. At birth, although this is now rare in developed countries. This is associated with obstructed or difficult deliveries.
Open injuries
In the past, cavalrymen wielding sabres disabled the enemy by cutting the upper cords of the brachial plexus of opposing infantry. Today, open injuries still occur and are just as devastating but they are more often caused by falling objects such as glass or steel.
Patterns of brachial plexus lesion
• Supraclavicular lesions, which can be (1) preganglionic or (2) postganglionic.
• Infraclavicular lesions.
Supraclavicular lesions
Trauma
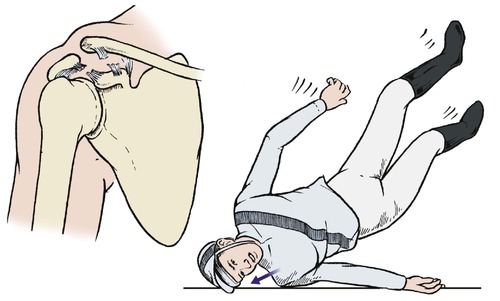
Blows to the shoulder and head cause violent lateral flexion of the cervical spine and depression of the shoulder. This tears the upper part of the brachial plexus. In the UK about 90% of these injuries occur in motorcyclists landing on the head and shoulder (Fig. 12.1).
 |
| Fig. 12.1 Traction injury of the brachial plexus. Violent abduction of the neck and shoulder can tear the upper cords of the brachial plexus. |
Obstetric palsy
If the upper cords of the plexus are damaged at birth, the supinator, deltoid, wrist extensors and elbow flexors will be weak, causing a ‘waiter’s tip’ position of the arm (Fig. 12.2). This condition is known as Erb’s palsy, a term which is often applied to the same pattern of neurological deficit in the adult.
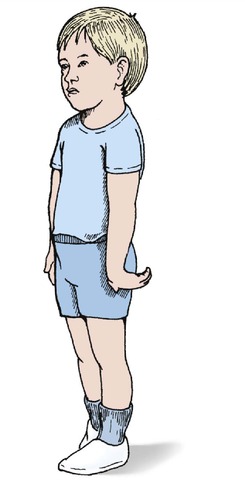 |
| Fig. 12.2 The position of the hand in Erb’s palsy. |
Infraclavicular lesions
Trauma
Injuries in which the arm is violently abducted can tear the lower part of the brachial plexus. The commonest mechanism is anterior dislocation of the shoulder, but the lesion can also be caused by a fall from a height in which the hand is caught so that the full weight is taken by the arm.
Birth trauma
The end result of damage to the lower cords of the brachial plexus at birth is a Klumpke’s palsy, which consists of a weakness of the finger flexors and intrinsics.
Assessment
The first step in management is to define the anatomy of the lesion. The roots, trunks or branches of the brachial plexus can be torn or the roots avulsed from the spinal cord. Each lesion has a different prognosis and the site of the lesion must be identified by a careful neurological examination.
The anatomy of the brachial plexus is so variable that trying to identify the exact site of the lesion using a map of the brachial plexus is most unreliable, but it does give a rough idea of the extent of the lesion (Fig. 12.3). In general terms, the more distal the lesion, the better the prognosis.
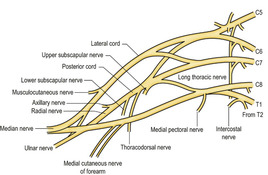 |
| Fig. 12.3 The brachial plexus. The anatomy is very variable. |
It is important to decide whether the lesion lies between the spinal cord and the dorsal root ganglion (preganglionic) or distal to the ganglion (postganglionic). Preganglionic lesions never recover, postganglionic lesions sometimes do.
One way of determining the exact site of the lesion clinically is to assess muscle function. The first branches to leave the brachial plexus are the motor nerves to the rhomboids and levator scapulae. If the patient has power in these muscles and can elevate the scapula, the lesion must be distal to the origin of these nerves from the plexus and the prognosis will be better than for a patient who cannot elevate the scapula.
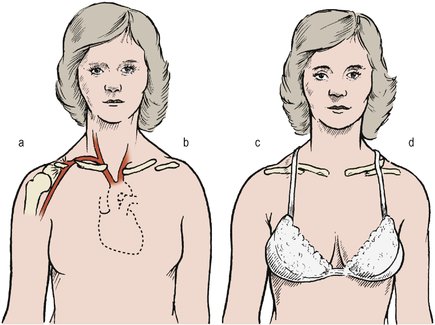
A useful approach is to look at the activity of the autonomic nervous system. If a Horner’s syndrome is present, the lesion must be close to the cord and the prognosis is poor (Fig. 12.4). Axonal reflexes involving the triple response or sweating can also be used. If axonal reflexes are present but the function of the dorsal root ganglion is absent, the lesion must be preganglionic and close to the cord.
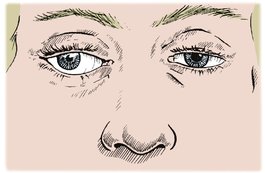 |
| Fig. 12.4 Horner’s syndrome, with drooping eyelid, small pupil, slight protrusion of the eyeball and no sweating of the surrounding skin. |
Investigations are less useful than clinical examination. The most useful investigation is the EMG, which can identify accurately the roots involved. Radiculography will show if the roots are still attached to the spinal cord and may demonstrate traumatic meningocoeles along the roots, but reveals little else. CT scanning does not give much information about the peripheral nerves, although MRI may prove helpful.
Treatment
If the roots are torn out of the spinal cord, nothing can be done to restore continuity. If the lesions are distal to the ganglion or there is a clean cut across the nerve, microsurgical repair may be possible. Cable grafting of defects in the supraclavicular part of the plexus is practised but the results are unpredictable, and a few patients eventually request amputation to rid themselves of their heavy, useless arm (p. 86).
Artificial limbs are available but many patients find them an encumbrance and do not wear them.
Management of brachial plexus lesions
1. Identify the site of the lesion by careful neurological examination and EMG.
2. Decide if the lesion is preganglionic or postganglionic.
3. Preganglionic lesions (Horner’s syndrome, absent axonal reflex) cannot be repaired.
4. Postganglionic lesions have a better prognosis: the more distal, the better the outlook.
5. Surgical repair or grafting is sometimes possible for clean cuts and distal lesions.
Injuries to the clavicle
A fractured clavicle is one of the commonest of all fractures. Clavicular injuries include (Fig. 12.5):
 |
| Fig. 12.5 Sites of fracture of the clavicle. |
1. Fracture of the midshaft of the clavicle.
2. Fracture of the outer end of the clavicle.
3. Acromioclavicular separation.
4. Sternoclavicular dislocation.
Fracture of the midshaft of the clavicle
The usual force that breaks a clavicle is a violent upwards and backwards thrust caused by landing on the outstretched hand or a direct blow to the point of the shoulder. This can happen after being thrown from a horse or going over the handlebars of a bicycle. The domestic cat does not have this problem because its clavicles are free at both ends (Fig. 12.6). Humans have clavicles firmly attached to the sternum medially and the acromion and coracoid laterally by ligaments that are stronger than the bone. The clavicle therefore fractures instead of moving to absorb the impact.
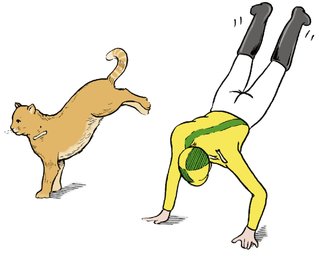 |
| Fig. 12.6 Falls on the outstretched arm. The cat does not fracture its clavicle because the sternum and humerus are not linked as in humans. |
The cat’s clavicle is adapted for landing on the forelegs but the forearms of humans are adapted for carrying weights. The human clavicle acts as a strut to hold the shoulder and arm away from the body, like a cantilever (Fig. 12.7). This function is only possible if the bone is intact; when the clavicle is broken the weight of the arm makes the fragments overlap and go on to malunion (Fig. 12.8).
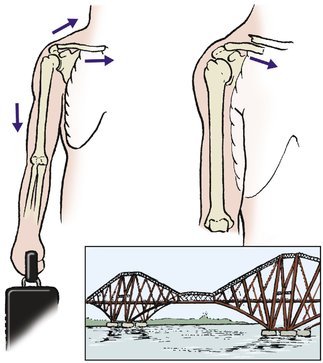 |
| Fig. 12.7 Cantilever action of the clavicle. When the clavicle is broken, the shoulder is not supported and moves downwards and medially. |
 |
| Fig. 12.8 Malunion of the clavicle with overriding bone fragments. |
In adults, a fractured clavicle takes about 6 weeks to become solid, although function returns after about 3 weeks. In children the fracture will be solid after only 2 or 3 weeks. If the fracture is comminuted, it will usually unite more quickly than a simple transverse fracture because there is more callus to ‘glue’ the bone ends together.
Complications
Complications are often seen after this injury (Fig. 12.9).
 |
| Fig. 12.9 Complications of fractured clavicle: (a) damage to the great vessels; (b) non-union; (c) malunion; (d) a spike of bone. |
Malunion. Because the fragments are displaced by the weight of the arm, malunion is unavoidable. Internal fixation with a contoured plate may give better anatomical results but the surgery has risks (neurovascular, skin etc.)
Damage to vessels. Splinters of bone can rupture the great vessels or the lung at the time of injury. It is said that Sir Robert Peel (the founder of the Metropolitan Police Force) died from this complication after being thrown by his horse.
Non-union is unusual and seldom causes symptoms. Internal fixation and grafting are required on the rare occasions when it does cause symptoms.
Deformity. Large spicules of bone around the fracture site can produce an unsightly appearance, as well as an unwelcome pressure area, and may need removing (Fig. 12.10).
 |
| Fig. 12.10 Malunion with an unsightly bony prominence at the site of fracture. |
The callus at the fracture site also produces a visible lump that interferes with the shoulder straps of bras and backpacks. The lump is particularly alarming to the parents of children with a greenstick fracture of the clavicle. The clavicle looks normal immediately after injury and the swelling may be mistaken for a malignant tumour. In time, the swelling diminishes as the bone remodels and the surrounding bone enlarges.
Treatment
A sling to support the weight of the arm relieves pain at the fracture site, but the sling must not rub against the fracture. The sling can be removed after 10 days if pain permits. Greenstick fractures require very little support (Fig. 12.11).
 |
| Fig. 12.11 Greenstick fracture of the clavicle. |
A firm support such as a figure-of-eight bandage to pull the shoulders backwards also helps to relieve pain but it must be readjusted every few days (Fig. 12.12). The function of a figure-of-eight bandage is to support the fracture and not to reduce it. Harnesses and braces that attempt to reduce the fracture by pulling the shoulder blades backwards are doomed to failure: the arm weighs several kilograms and anything that exerts such a force on the shoulder is bound to cause pressure sores in the soft axillary skin, even without the sweat that is inevitable under a bulky dressing.
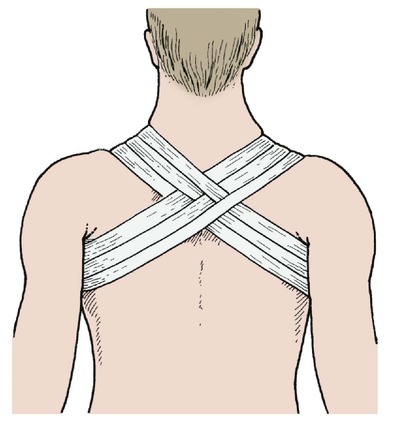 |
| Fig. 12.12 Figure-of-eight bandage for fractured clavicle. |
Internal fixation is seldom required for fractures of the clavicle.
Fractures of the outer end of the clavicle
Fractures of the outer end of the clavicle lie lateral to the coracoclavicular ligament and the distal fragment remains attached to the acromion. Fractures may involve the acromioclavicular joint and may be displaced or undisplaced.
Thus, the fractures can be classified as displaced or undisplaced and articular or non-articular.
Treatment
Undisplaced non-articular fractures are treated conservatively with a sling, analgesics and early mobilization.
Complications
The fragment may fail to unite, causing a painful non-union. Excision of the un-united fragment may be needed if this occurs.
Acromioclavicular separation
The acromioclavicular joint is a plane joint between the end of the clavicle and the acromion. It contains a fibrocartilaginous disc and is easily disrupted by a fall onto the point of the shoulder (Fig. 12.13). The injury is sometimes called a ‘separated’ or ‘sprung’ shoulder and occurs in rugby football, riding accidents and ice hockey if the shoulder is struck against the boards around the rink. The lesion is usually a simple dislocation of the joint but a fragment of the clavicle sometimes remains attached to the acromion.
 |
| Fig. 12.13 Fracture of the acromioclavicular joint. Falling onto the point of the shoulder can rupture the coracoclavicular ligament. |
Clinical examination will show tenderness of the acromioclavicular joint and a step at the joint, best seen when the arm is allowed to hang. The step can be eliminated by lifting the arm and the elbow while holding the clavicle down.
Grading and treatment
There are six grades of acromioclavicular separation. The grade determines the treatment:
1. Sprain with no displacement. Analgesics and symptomatic treatment only.
2. Subluxation. Treatment consists of analgesia and, if necessary, a sling to support the elbow.
3. Dislocation. Complete separation of the joint usually requires internal fixation.
4. Dislocation with perforation of the overlying deltotrapezius fascia. Open reduction with internal fixation and repair of the fascia may be needed.
5. Lesions described in (4) above with the addition of posterior dislocation. Open reduction and internal fixation is required for this serious injury.
6. Subcoracoid dislocation. Open reduction and internal fixation is required for this serious injury, which involves the scapula.
Sternoclavicular dislocation
The sternoclavicular joint lies medial to the stout costoclavicular ligament that acts as a pivot for the clavicle, which see-saws about this point. When the outer end of the clavicle is raised, the medial end moves downwards, and vice versa – confirm this by putting a finger on the medial end of the clavicle and moving the shoulder.
Treatment
If the injury is seen early, which is unusual, acute repair may be required. The decision to operate depends on the age and fitness of the patient and the severity of the injury. Left untreated, recurrent subluxation can occur. Soft tissue repair is difficult and the patient may prefer to accept the minor disability of recurrent subluxation instead.
Fractures of the scapula
Fractures of the acromion
The acromion can be broken by direct trauma or by violent abduction of the shoulder (Fig. 12.14). It is easy to confuse the normal apophysis of the acromion in the growing skeleton with a fracture, and many a normal acromioclavicular joint has been ‘treated’ in a sling for this reason.
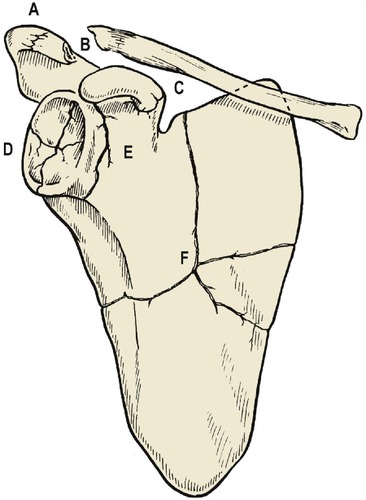 |
| Fig. 12.14 Sites of fracture of the scapula: ( A) acromion; ( B) fracture dislocation of the acromioclavicular joint; ( C) coracoid; ( D) glenoid; ( E) neck of scapula; ( F) blade of scapula. |
Treatment
Acromioclavicular injuries with little separation and intact coracoclavicular ligaments require no treatment. Rest in a sling is sufficient unless there is gross displacement of the fragments, when internal fixation may be needed to stabilize the joint.
The blade of the scapula
The blade of the scapula, like the wing of the ilium, functions mainly as an attachment for muscles. It can be fractured by direct trauma, causing pain, bruising and soft tissue swelling.
Treatment
Treatment is by support in a sling, analgesics and early mobilization. A good result is usual, but the shoulder girdle may be weaker than before because of muscle damage.
The glenoid
The glenoid can be fractured by a direct blow to the shoulder from the lateral side, comparable with the force which causes a fracture of the floor of the acetabulum.
Treatment
Unless there is gross displacement of the fragments, treatment is by early mobilization. Because the glenoid is not a weight-bearing joint, exact anatomical restitution of the joint surfaces is less important than early mobilization.
Dislocation of the shoulder
The shoulder is mechanically unstable. The head of the humerus is held against the glenoid by a cowl of muscles that pull the round head of the humerus up against the small flat glenoid, which faces downwards. The cowl of muscles is complete everywhere except below, in the axilla, where there is nothing to hold the humeral head against the glenoid. Bearing this intrinsic instability in mind, it is remarkable that dislocation is not more common.
There are five types of shoulder dislocation:
1. Anterior dislocation.
2. Posterior dislocation.
3. Luxatio erecta, or true inferior dislocation.
4. Fracture dislocations.
5. Multidirectional.
Anterior dislocation
Anterior dislocation is by far the commonest pattern and is the result of the head of humerus slipping off the front of the glenoid when the arm is abducted and externally rotated (Fig. 12.15). The shoulder can also dislocate during grand mal attacks or electroconvulsive therapy and may then pass unnoticed for some days.
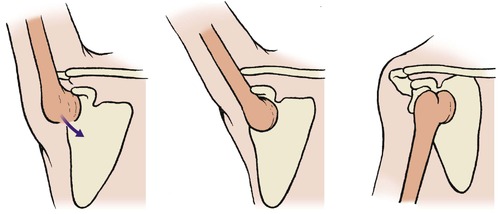 |
| Fig. 12.15 Mechanism of anterior dislocation of the humerus, beginning with abduction and extension. |
Once off the glenoid, the head slips medially when the arm is lowered, producing the characteristic profile of a dislocated shoulder. Because the head of the humerus is not lying in its normal position, the shoulder has a flatter appearance than usual and the elbow points outwards. If the tip of the acromion and the lateral epicondyle can be joined by a straight line (Hamilton’s ruler test), the shoulder is dislocated (see Fig. 2.13).
This appearance, together with the observation that the patient is holding the injured arm in the other hand, makes it possible to diagnose a dislocated shoulder from the far end of the accident department. A similar flattened contour is also seen in patients with wasted deltoid muscles and in displaced fractures of the surgical neck, but in these patients the humeral head is still in its normal position and the ‘ruler test’ is negative.
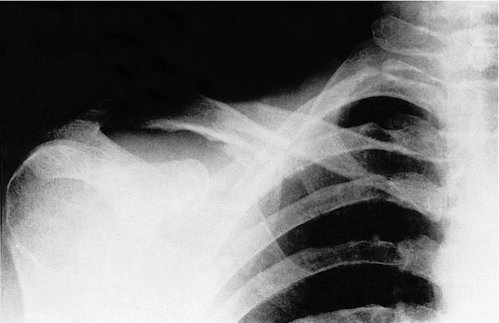
Radiographic examination of a dislocated shoulder is not easy (Fig. 12.16). It is difficult to position the patient accurately and the usual lateral film in abduction is impossible, but an axial view will reveal the dislocation. A lateral scapula view is excellent. Fractures of the humeral head should be looked for specifically, or they will be missed and a fracture dislocation will be treated as a simple dislocation, with potentially serious clinical and medicolegal consequences.
 |
| Fig. 12.16 Dislocation of the shoulder with separation of the greater tuberosity. |
Complications
Complications of anterior dislocation of the shoulder
• Damage to the circumflex axillary nerve.
• Arterial damage.
• Irreducibility.
• Joint stiffness.
• Recurrent dislocation.
Neurological damage. Damage to the axillary nerve as it runs round the neck of the humerus (Fig. 12.17) causes partial or complete paralysis of the deltoid. When damage is suspected, the axillary nerve should be examined with an EMG 3 weeks after injury and again 3 weeks later. If there is no change between the two examinations, the nerve should be explored and, if necessary, repaired.
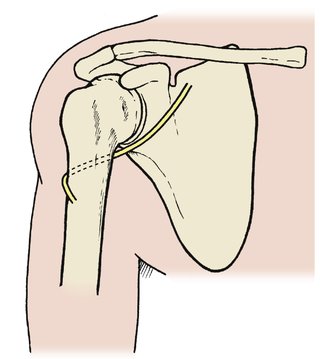 |
| Fig. 12.17 To show the relationship of the circumflex humeral nerve to the deltoid and the surgical neck of the humerus. |
Brachial plexus injuries also occur if there has been a violent abduction strain.
Arterial injury. The axillary artery can be damaged by traction at the time of injury or by pressure from the humeral head. The radial pulse should be checked and its presence recorded.
Irreducibility. The humeral head sometimes ‘buttonholes’ through the subscapularis, making reduction impossible. Open reduction is then necessary.
If the shoulder is not reduced within a few days of dislocation, reduction may then be impossible. This is a particular problem in elderly patients in whom the shoulder can be dislocated with trivial trauma. Open reduction is a difficult and uncertain operation and it may be better left dislocated in an elderly patient who places little demand on the shoulder.
Joint stiffness. Because the shoulder depends upon muscle and soft tissue for stability, adhesions or fibrosis in the rotator cuff can cause serious loss of movement. Physiotherapy is important to prevent this.
Recurrent dislocation. Once dislocated, the shoulder is liable to do so again and may require stabilization. Adequate treatment of the initial dislocation is therefore important.
Treatment
First, examine the shoulder radiologically, however obvious the diagnosis may be. Attempts to reduce the shoulder before radiographs are available are ill advised and may be dangerous if there is an associated fracture.
The humeral head must be reduced but, before attempting reduction, test the function of the axillary nerve, which runs around the surgical neck of the humerus. This nerve can be damaged either at the moment of dislocation or during reduction. Because the nerve is so vulnerable, it is important to test the function of the nerve and record it before reduction is attempted.
Motor function cannot be tested adequately but the area of sensory supply of the circumflex nerve, over the outer side of the deltoid, is easily tested. If there is any abnormality it should be clearly recorded and special care taken when the shoulder is reduced. If this is not done, any subsequent circumflex nerve dysfunction may be attributed to the reduction rather than the injury.









