Chapter 14. Injuries to the lower limb
Fractures at the upper end of the femur: general considerations
Fractures at the upper end of the femur are seen in young patients and high energy injuries or in elderly patients with bones weakened by osteoporosis. Because they live longer than men and the hormonal changes of the menopause make them more subject to osteoporosis, these fractures are commoner in women. The fractures are becoming more and more frequent as the average age of the population increases and in many areas they are the commonest fractures admitted to hospital.
Fractures at the upper end of the femur create clinical, social and economic problems.
Clinical problems
Because the fractures occur in elderly patients, medical problems are seen that are not encountered in fit young adults with broken bones or in older patients undergoing reconstructive surgery. Assessment therefore requires special attention to the general medical condition, drugs that the patient is taking and the social history.
Bronchopneumonia and cerebral confusion are particular problems and the prognosis for an elderly patient with a fracture at the upper end of the femur is poor.
Approximately 10% of patients die within 6 weeks of this injury and 30% within 1 year.
Of the remaining 70% who survive, one-third are unable to return to their former level of independence or physical activity as the result of the fracture.
Social problems
The fractures are important from the social stand-point because they often connote the end of independent existence, particularly if the patient has unsuitable accommodation and was unfit to live alone even before the fracture. Admission to hospital – a strange and frightening place for an elderly patient at the best of times – always causes anxiety which, when coupled with the upset of operation, may be so great that the patient is quite unable to cope with the problems of rehabilitation.
If return home is impossible and alternative accommodation has to be found, close liaison with the social services, family practitioner and health visitor is mandatory (p. 88). The mental adjustment asked of the patient will be even greater and this must be taken into consideration.
Economic problems
These fractures consume a large part of health service resources in terms of beds, nurses and support outside hospital. As the fractures become more common, pressure on resources becomes greater but there is seldom any increase in the provision of services to match the increased demand.
The result is more pressure on less urgent services, which in practice means that patients with non-urgent conditions cannot be treated and must wait longer for admission to hospital. The level of provision for fractured necks of femur is largely responsible for long orthopaedic waiting lists.
Fractures of the femoral neck
Fractures of the acetabulum are dealt with on page 000.
Clinical features
Fractures of the femoral neck occur after a trivial injury or even without any injury at all; the bone may be so brittle that it snaps as the patient gets out of a chair.
On examination, the affected leg will be short and externally rotated because the fracture allows the shaft of the femur to move independently of the hip joint, which means that the iliopsoas and gravity will rotate the femur externally instead of rotating the hip internally (Fig. 14.1).
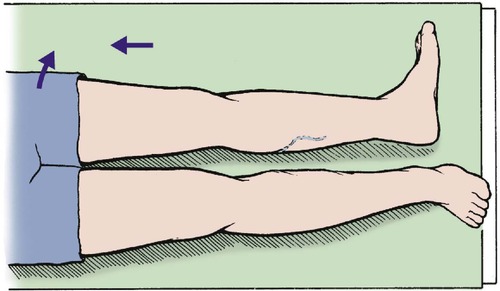 |
| Fig. 14.1 Position of the leg with shortening and external rotation, seen with a displaced fracture at the upper end of the femur. |
Types of fracture
Intracapsular fractures result from a high transcervical fracture and interrupt the blood supply to the femoral head. This is derived from three sources (Fig. 14.2).
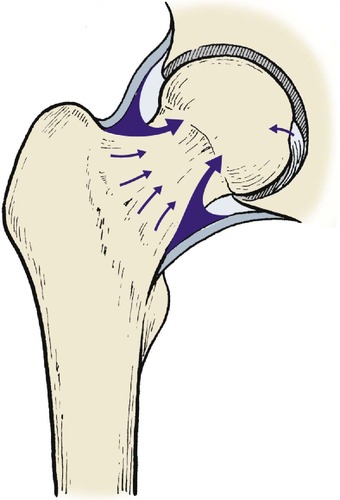 |
| Fig. 14.2 Blood supply of the femoral head via the capsule, intramedullary vessels and ligamentum teres. |
Blood supply to the femoral head
1. Synovium and joint capsule.
2. The medullary cavity.
3. A tiny proportion from the ligamentum teres.
An intracapsular fracture can cut off the blood supply to the femoral head completely, leading to aseptic necrosis, non-union, or both. Because the fracture line is inside the capsule, blood is contained within it. This raises the intracapsular pressure and damages the femoral head still further. It also prevents visible bruising because blood cannot reach the subcutaneous tissues.
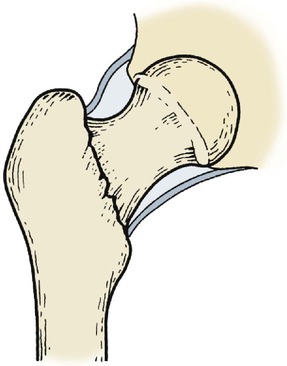
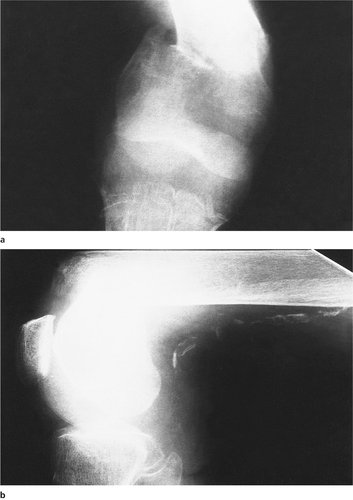
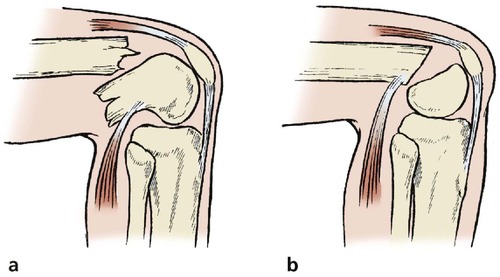
To add to these problems, an intracapsular fracture leaves the femoral head very mobile inside the capsule (Fig. 14.3 and Fig. 14.4), particularly if the fracture is just below the head (subcapital). This makes accurate reduction almost impossible. The posterior cortex may also be crushed.
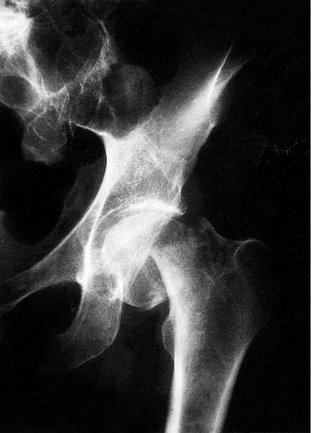 |
| Fig. 14.3 Displaced subcapital fracture of the femoral neck. The femoral shaft has moved proximally. |
 |
| Fig. 14.4 Displaced transcervical fracture of the femoral neck. The femoral head maintains its correct relationship to the pelvis but the femur is rotated. |
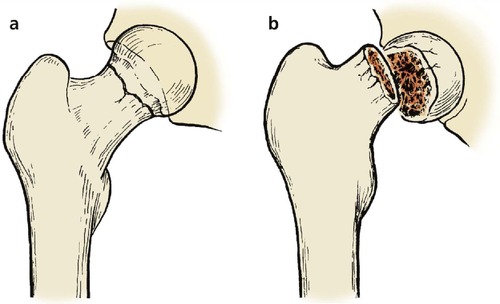
All these factors predispose to non-union and aseptic necrosis (Fig. 14.5), and intracapsular fractures are notorious for their high complication rate.
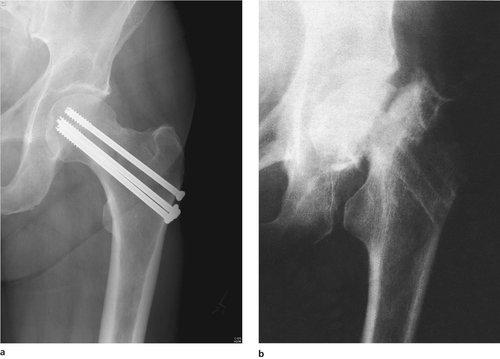 |
| Fig. 14.5 (a) Internal fixation of a femoral neck fracture with screws. (b) Non-union of a femoral neck fracture with aseptic necrosis of the femoral head. Note how the head has become smaller and denser. |
Extracapsular and basal fractures are less difficult for three reasons (Fig. 14.6):
1. The blood supply is not interrupted so seriously.
2. The surface area of the fracture available for union is larger and consists of good cancellous bone.
3. The femoral head is less mobile.
 |
| Fig. 14.6 Basal fracture of the femoral neck. |
Nevertheless, non-union and avascular necrosis can occur, and extracapsular fractures must be treated with great respect.
Undisplaced and impacted fractures of the femoral neck present other problems (Fig. 14.7, Fig. 14.8 and Fig. 14.9). Because the bones are jammed tightly together the fracture appears stable and the patient may even be able to bear weight on the leg (Fig. 14.10). Many impacted fractures probably pass undiagnosed and do very well without medical attention, but in some patients the fracture becomes displaced days or even weeks after the injury. An impacted fracture must therefore be carefully observed to be certain that it remains stable, and should be protected until the bones are united.
 |
| Fig. 14.7 Impacted fracture of the femoral neck with the head in valgus. |
 |
| Fig. 14.8 Impacted fracture of the femoral neck. The head rolls into valgus and there is double density of the bone at the site of impaction. |
 |
| Fig. 14.9 (a) Undisplaced fracture of the femoral neck; (b) displaced fracture of the femoral neck. |
 |
| Fig. 14.10 Impacted fracture of the femoral head with little valgus deformity. The patient had walked on this fracture. |
Treatment (intracapsular)
The choice of treatment for femoral neck fractures depends upon three factors:
1. The age and fitness of the patient.
2. The type of fracture.
3. The degree of displacement.
Displaced fractures can be treated by internal fixation or prosthetic replacement.
Internal fixation. The fracture can be held with several fine pins, a pair of crossed nails, cannulated screws or a dynamic compression screw and plate. All of these are inserted under image intensifier control (Fig. 14.11).
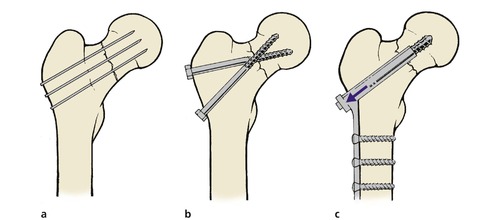 |
| Fig. 14.11 Methods of internal fixation of femoral neck fractures: (a) multiple pins; (b) crossed screw-nails; (c) compression with dynamic screw and plate. |
The fracture must be protected from full weight-bearing after fixation, which is difficult in the elderly patient, who may not be able to use crutches easily.
If successful, internal fixation of the fracture produces an almost perfect hip, but if the fracture is complicated by aseptic necrosis or non-union, a second operation will be required to replace the head with a prosthesis (Table 14.1). The femoral head may also collapse onto the pins, damaging the acetabulum.
| Indications |
| Internal fixation: fit; young, little displacement |
| Prosthesis: unfit, old, displaced fractures |
| Results |
| Internal fixation: better long-term result. More complications. May need second operation. Slow rehabilitation |
| Prosthesis: early mobilization. Long-term complications are rarer but more serious. A good guideline is to fix the fractures of fit patients under 65 and replace the rest |
Prosthetic replacement. Immediate replacement of the head with a hemiarthroplasty (e.g. Thompson or Austin Moore prosthesis; Fig. 14.12) avoids the complications of non-union and aseptic necrosis and allows immediate full weight-bearing (Fig. 14.13).
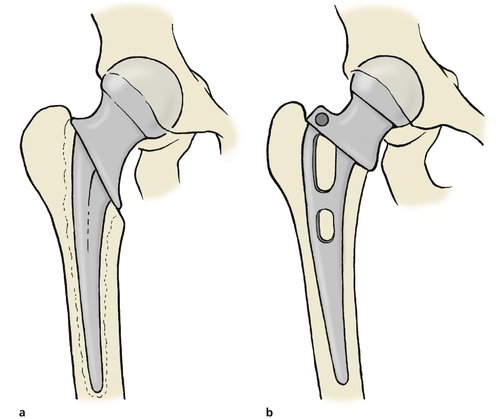 |
| Fig. 14.12 Hip prosthesis for fracture of the femoral neck: (a) Thompson prosthesis secured with cement; (b) Austin Moore prosthesis with no cement. |
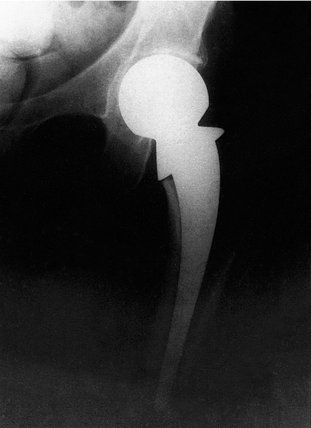 |
| Fig. 14.13 A Thompson prosthesis in position. |
Early mobilization has many advantages, but the prosthesis may loosen or the femoral head may erode the floor of the acetabulum. If either complication occurs, a total hip replacement will be needed. The wound may also become infected, making excision arthroplasty necessary.
As always with prosthetic replacement, the results are better than other techniques when they are successful but far worse when they are not.
Bipolar prostheses. ‘Bipolar prostheses’ are useful in younger patients. A bipolar prosthesis includes a ball and socket bearing within the space occupied by the femoral head. Thus, the outside diameter of the prosthesis replaces the femoral head and fills the acetabulum. Within this sphere there is a second bearing, usually about 22 mm in diameter. Ball and socket movement can therefore occur at two joints, the interface between the acetabulum and the outer circumference of the prosthesis and the smaller bearing within.
These prostheses are more expensive than simple femoral prostheses but they reduce the forces imposed on the interface between the outer circumference and the acetabulum. They are particularly suitable for younger patients with femoral neck fractures not suitable for internal fixation.
Trochanteric fractures
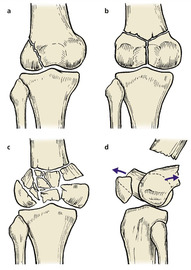
There are four types of trochanteric fracture (Fig. 14.14):
1. Pertrochanteric – through both trochanters.
2. Intertrochanteric – between the trochanters.
3. Subtrochanteric – below the trochanters.
4. Avulsion of the trochanters.
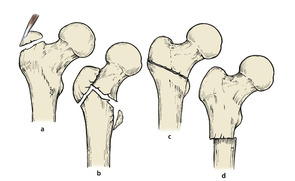 |
| Fig. 14.14 Types of trochanteric fracture: (a) avulsion of the greater tuberosity; (b) pertrochanteric fracture; (c) intertrochanteric fracture between the trochanters; (d) subtrochanteric fracture. |
Pertrochanteric and intertrochanteric fractures
Clinical features
In contrast to fractures through the femoral neck, which occur with little or no trauma, these fractures are caused by a sharp twisting injury, and a history of trauma is usual (Fig 14.15). A further point of difference is that fractures of the femoral neck do not occur in joints affected by osteoarthritis because osteoarthritic bone is denser than normal and the femoral neck is not the weakest point.
 |
| Fig. 14.15 Pertrochanteric fracture of the femur following a fall. |
Fractures through or between the trochanters present different problems from those of the femoral neck. Because the fractures occur through cancellous bone and are surrounded by muscle, they almost always unite but are very unstable and malunion is almost inevitable unless they are fixed internally.
Treatment
Pertrochanteric or intertrochanteric fractures must be held in good position, preferably with a dynamic hip screw or intramedullary hip screw, until united (Fig. 14.16). These implants are not strong enough to take over the mechanical functions of the femur and allow the patient to put all his or her weight through the limb, but they will hold the bones together for the 8 weeks or so needed for union to occur.
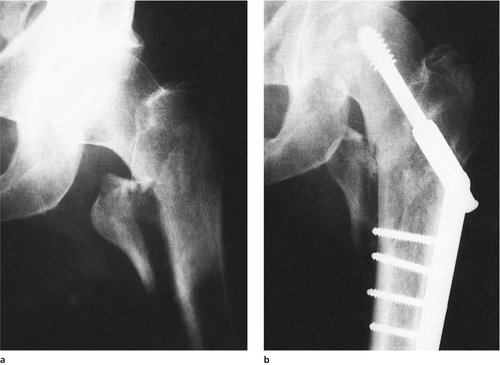 |
| Fig. 14.16 (a), (b) Pertrochanteric fracture fixed with compression screw and nail-plate. |
Subtrochanteric fractures
Subtrochanteric fractures are rarer than fractures of the neck or pertrochanteric fractures and are often pathological, occurring through areas of Paget’s disease or metastases (Fig. 14.17a).
 |
| Fig. 14.17 (a) Subtrochanteric fracture through an area of Paget’s disease. (b) Subtrochanteric fracture with intramedullary nail. |
Treatment
Subtrochanteric fractures usually require internal fixation using a nail-plate with a long femoral plate or an intramedullary implant (Fig. 14.17b). If the fracture is pathological, the underlying disorder will also need attention.
Avulsion of the greater trochanter
The greater trochanter can be avulsed by a violent adduction strain.
Clinical presentation
The patient experiences severe pain over the trochanter, abduction is painful and the Trendelenburg sign (p. 25) is positive because the abductor muscles are separated from their bony attachment.
Treatment
Large fragments with much displacement should be reattached if the patient is fit enough but many patients achieve a good result without internal fixation. Non-union is common and causes marked weakness of the abductors, with a Trendelenburg gait.
Fractures at the upper end of the femur in children
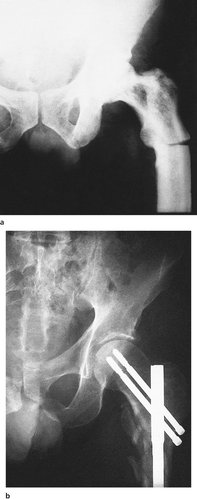
Slipped upper femoral epiphysis
In children, the anatomical equivalent of an intracapsular fracture of the femoral neck is a slipped upper femoral epiphysis (Fig. 14.18). The condition occurs most often during the adolescent growth spurt, is commoner in boys than girls, and consists of a medial and backward displacement of the epiphysis, which rolls the limb into external rotation. The slip is either as a result of a Salter I fracture due to trauma or as an insidious gradual event. The slip is probably the result of weakening of the epiphyseal plate and soft tissues by the hormones of adolescence and this may explain why plump gynaecoid boys are most often affected.
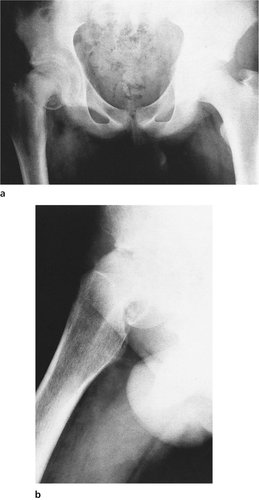 |
| Fig. 14.18 Slipped upper femoral epiphysis: (a) anteroposterior view; (b) lateral view. |
Clinical features
A slipped upper femoral epiphysis often causes referred pain to the knee and the diagnosis should be suspected in any adolescent with aching around the knee but no abnormality at the knee on clinical examination.
On examination, the appearance is very like that of a femoral neck fracture, the leg lying shortened and externally rotated. The condition is bilateral in 40% of cases and the opposite hip should therefore be checked.
Complications
A slipped upper femoral epiphysis can be followed by avascular necrosis of the epiphysis and early osteoarthritis, or by necrosis of the articular cartilage, which also leads to a stiff and painful hip.
Treatment
Slight or moderate displacement should be treated by fixation with pins to prevent further slip.
Manipulation or traction, however gentle, may cause aseptic necrosis of the epiphysis and should not be attempted. Do not manipulate a slipped upper femoral epiphysis. Although this was once standard practice it is now thought to cause further damage to the epiphysis and its blood supply.
Gross displacement may be irreducible, particularly if there is a long history. In these patients it may be better to accept the deformity and correct it by osteotomy when growth is complete, although there is a high incidence of aseptic necrosis of the head.
Femoral neck fractures
Fractures at the upper end of the femur are essentially an injury of the elderly but they are seen very occasionally in children, when they behave very differently. The fractures are usually basal and the prognosis is worse than in adults.
Although rare, these fractures are serious when they occur and the entire femoral head and neck may undergo aseptic necrosis.
Fractures of the femoral shaft
The femoral shaft can be fractured by direct trauma, twisting or a blow to the front of the flexed knee in a road traffic accident. This injury can also produce a fracture of the patella, ruptured posterior cruciate ligament and posterior dislocation of the hip.
Clinical features
A broken thigh is shorter and fatter than normal and lies with the distal fragment in external rotation and adduction for four reasons (Fig. 14.19):
1. Without the longitudinal stability of the femur, the muscles attached to the upper and lower ends contract and the thigh shortens, which makes it look swollen (Fig. 14.20).
 |
| Fig. 14.20 Swelling of the thigh in a patient with a fracture of the femur. An inflatable air splint has been applied for a fracture of the tibial shaft. |
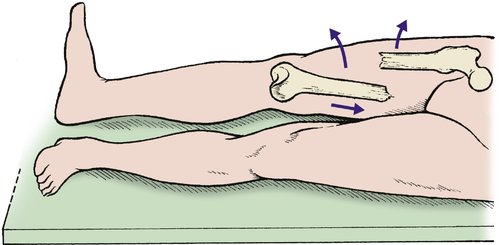 |
| Fig. 14.19 Position of the fragments after a fracture of the femoral shaft. The upper fragment swings upwards and outwards, the distal fragment is adducted and the foot is externally rotated. |
2. The adductors are attached to the distal fragment and the abductors to the upper fragment. The fracture separates the two groups, which then act unopposed (p. 39).
3. The weight of the foot rolls the distal fragment into external rotation.
4. The femur is surrounded by muscle which is lacerated by the sharp ends of the fractured bone and the thigh fills with blood. The bone also bleeds.
Complications
• Haemorrhage, which can lead to cardiovascular collapse. This can be corrected by adequate transfusion.
• Infection, particularly if a wound is contaminated and wound debridement has been inadequate.
• Non-union, which is common in midshaft fractures, high speed trauma and fractures with soft tissues interposed between the fragments. Non-united fractures need bone grafting and internal fixation.
• Malunion, caused by abductors and adductors acting unopposed on the proximal and distal fragments, respectively. A varus deformity results from this combination of forces.
• Arterial and nerve injury is uncommon but does occur. The neurological and vascular state of the foot should always be checked and recorded.
Treatment
Immediate care
The blood loss from a fractured femur, whether open or closed, is between 2 and 4 units (1–2 litres). An intravenous line should therefore be set up and blood sent to the laboratory for haemoglobin estimation and cross-matching. If there are no other fractures, it may be possible to avoid transfusion, but if any other injuries are present, 2 units of blood should be given as soon as it is available.
Open fractures are usually open from within out, with a wound on the lateral side or the front of the thigh. The wound should be debrided meticulously in the operating theatre and all foreign material removed. It is usually wise to pack the wound and treat it by delayed primary suture (p. 139). Only in very exceptional circumstances can a wound be made clean enough to close immediately. Antibiotics and antitetanus treatment should be given, as for any open fracture.
Treatment of the fracture
When the patient’s condition is stable and the wound has been dealt with, the fracture can be immobilized in one of four ways:
1. Traction.
2. Internal fixation.
3. External fixation.
4. Cast bracing.
Traction. Traction used to be the mainstay of treatment of these fractures in the past. Patients were in bed for up to 3 months at times. Traction is now rarely used and is only advocated when surgery is contraindicated or in children. A single, balanced, skeletal traction apparatus is shown applied via a femoral pin in Figure 14.21.
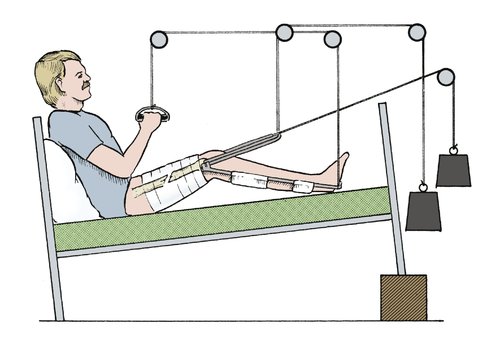 |
| Fig. 14.21 Conservative treatment of a femoral shaft fracture with balanced sliding traction and a knee flexion piece. |
Adequate longitudinal traction is needed for the first 24 h to overcome muscle spasm and prevent shortening and the fragments must be supported posteriorly to prevent sagging. Six kilograms (131b) is usually enough, but heavy patients need more and light patients less. Check radiographs after 24 h will show if the weight is correct; if there is overdistraction, the weight should be reduced. If there is overlap, it should be increased.
Internal fixation. An intramedullary nail is ideal for most fractures (Fig. 14.22). Fractures can be held straight and out to length by a nail, but the fixation may not be firm enough to control rotation. The advent of locking nails – where screws are inserted through the bone and nail – can now control rotation. Open reduction and fixation with a plate is not often performed owing to the extensive soft tissue exposure needed, the devitalization of the bone, and the mechanical failure of the plates.
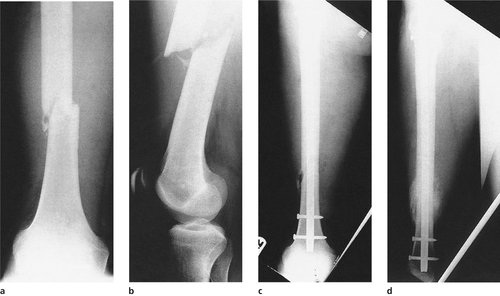 |
| Fig. 14.22 Unstable fracture of the femur: (a), (b) before operation; (c) after fixation with a locking nail; (d) united with callus. |
The advantages of intramedullary nailing are that it provides longitudinal stability as well as alignment and enables the patient to be mobilized rapidly enough to leave hospital within days of fracture. Disadvantages include the anaesthetic, additional surgical trauma and the risk of infection.
Intramedullary nails are inserted through the proximal or distal femur. They can be ‘reamed’ or ‘unreamed’. This simply means that the medullary cavity of the bone is enlarged to allow the nail to fit into the bone. The theoretical advantage of unreamed nails is that there is no excessive damage to the endosteal blood supply, which may further weaken the bone. By reaming the intramedullary canal, the intact endosteal blood supply is damaged throughout the length of the reamed segment and this, in conjunction with the damage to the periosteal layer, may delay healing.
Intramedullary nails can be used for comminuted fractures with shortening, provided the bone can be pulled out to length and held there. Locking nails which maintain length and rotation (p. 135) are required for such fractures.
External fixation. External fixation is used for contaminated and unstable open fractures or in the emergency situation.
Cast bracing. When a fracture treated on traction is stable and a mass of callus is visible radiologically, usually at about 6 weeks, a cast brace can be applied. Fractures in which fixation is less than 100% secure are also suitable.
The cast brace (p. 131) will enable the patient to leave hospital and begin rehabilitation more rapidly.
Fractures of the lower end of the femur
Supracondylar fractures
Supracondylar fractures are commonest in older patients with soft porotic bone (Fig. 14.23). The fractures are caused by either forced flexion or hyperextension and are unstable. Gastrocnemius flexes the distal fragment and increases the deformity (Fig. 14.24).
 |
| Fig. 14.23 (a), (b) Supracondylar fracture of the femur in an elderly patient. Note the calcification in the femoral vessels and the extreme flexion of the distal fragment. |
 |
| Fig. 14.24 Injuries of the lower end of the femur: (a) the mechanism of flexion of the distal fragment in a supracondylar fracture; (b) slipped lower femoral epiphysis. |
Treatment
These fractures are difficult to control conservatively because of the mobility of the distal fragment. Internal fixation is the method of choice. A blade or dynamic compression screw can be used and the newer locking plates may be of value in the porotic bone. An intramedullary implant, when inserted through the intercondylar notch of the femur, will hold the bone out to length and in the reduced position. This can be supplemented with additional screws to hold fragments together.
Slipped lower femoral epiphysis
In children, the equivalent of a supracondylar fracture is a slipped lower femoral epiphysis caused by a sharp flexion injury. Surgeons of the 19th century recorded that the fracture occurred in boys who fell backward while sitting on railings or whose feet became caught in the spokes of the wheel while riding on the back of a horse-drawn cart. Today, these injuries are less common.
Treatment
Reduction is usually easy but accuracy is important because angular deformities occur if the reduction is not perfect or the epiphysis is damaged.
Comminuted fractures
Violent trauma, particularly from motor cycle accidents, produces a very nasty comminuted fracture just above the condyle, often accompanied by a condylar fracture. The comminution is usually so great that the bone fragments cannot be reassembled and bone length is lost.
Treatment
Traction or external fixation may hold the bone out to its correct length but grafting may be required to fill the defect. Circular frames with wire fixation may hold the fragments. Again, locking plates may be of use.
Condylar fractures
Fractures entering the intercondylar notch can break one or both condyles away from the femoral shaft, or follow an oblique line (Fig. 14.25). The relationship of the two condyles is essential for normal knee function and accurate reduction is important; even a millimetre of proximal displacement leaves a valgus or varus deformity and rotation of one condyle relative to the other interferes with flexion.
 |
| Fig. 14.25 Fractures of the femoral condyles: (a) oblique fracture of the lateral condyle; (b) Y-shaped fracture into the notch; (c) comminuted fracture with (d) rotation of the condyles. |
Treatment
Treatment depends on the degree of displacement.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


