CHAPTER 17 Indications and Contraindications
The use of unconstrained humeral head replacement in acute fracture cases represents perhaps the most difficult indication for shoulder arthroplasty. Patients who are candidates for arthroplasty after proximal humeral fracture tend to be older with age-related osteopenia. Complications, both systemic and shoulder specific, are more common in this patient population than in patients undergoing unconstrained shoulder arthroplasty for chronic conditions. These factors contribute to the difficulty in treating proximal humeral fractures with unconstrained shoulder arthroplasty.
Neer popularized the use of humeral head replacement for the treatment of complex proximal humeral fractures.1 Neer’s classification of these fractures is the most commonly used scheme. Unfortunately, this classification system has been shown to have poor interobserver and intraobserver reliability.2 Other classification schemes have been introduced, but their complexity has limited their usefulness. For us, the most important, readily observable factor that indicates the need for shoulder arthroplasty after proximal humeral fracture is the condition of the humeral head articular fragment (soft tissue attachments, bone quality, dislocation, head splitting). In all cases in which we are anticipating possible shoulder arthroplasty for the treatment of proximal humeral fracture, we obtain a computed tomogram. Because of the widespread use of Neer’s classification scheme, this chapter discusses our indications for unconstrained shoulder arthroplasty based on the condition of the humeral head fragment within the context of the Neer classification as determined by computed tomography.
FOUR-PART PROXIMAL HUMERAL FRACTURES
The most common indication for unconstrained shoulder arthroplasty for proximal humeral fracture is a “four-part” fracture. This refers to a fracture involving four distinct fragments, including a humeral head fragment, a greater tuberosity fragment, a lesser tuberosity fragment, and a humeral shaft fragment (Fig. 17-1). Neer did not consider a fragment to constitute a “part” unless it was displaced greater than 1 cm or angulated more than 45 degrees.1 We have found strict application of these criteria to be difficult because determination of fragment angulation and even displacement can be complex despite the use of computed tomography. In any fracture that contains fracture lines separating the proximal humerus into four parts for which we plan operative treatment consisting of open reduction and internal fixation, we will be prepared to perform a hemiarthroplasty should the need arise intraoperatively. The two principal circumstances that make us opt for hemiarthroplasty, even in cases in which the tuberosities are displaced less than 1 cm, are when the humeral head fragment is discovered to be completely devoid of soft tissue attachment (Fig. 17-2) and when the bone in the humeral head is too severely osteopenic to permit any sort of fixation. In cases in which each fragment is clearly displaced more than 1 cm, we plan to perform hemiarthroplasty from the outset (Fig. 17-3).
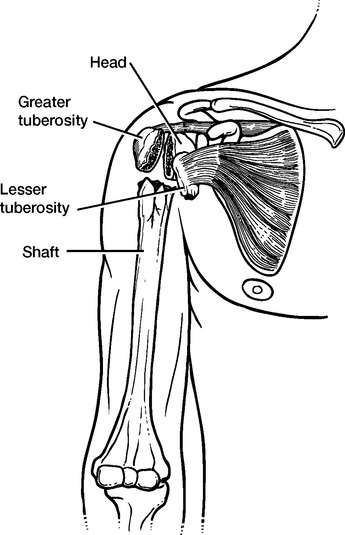
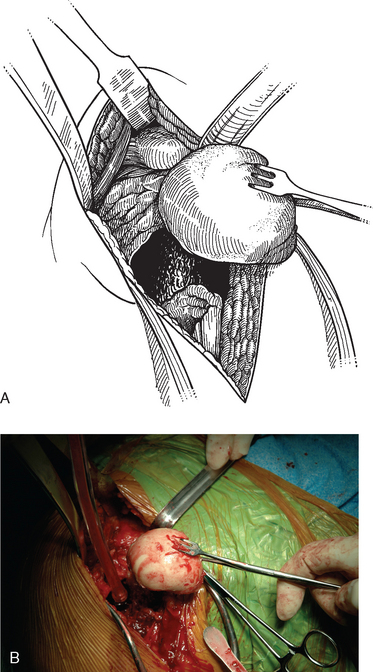
Figure 17-2 A and B, Drawing and intraoperative photograph of a humeral head devoid of soft tissue attachment.

THREE-PART PROXIMAL HUMERAL FRACTURES
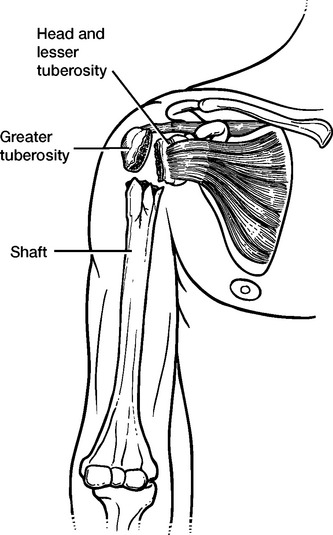
A less common indication for unconstrained shoulder arthroplasty for the treatment of proximal humeral fracture is a “three-part” fracture. This refers to a fracture involving three distinct fragments, including a humeral head fragment, a greater (more common) or lesser (less common) tuberosity fragment, and a humeral shaft fragment (Fig. 17-4). The majority of these fractures can be treated successfully with open reduction and internal fixation. In any fracture that contains fracture lines separating the proximal humerus into three parts for which we plan operative treatment consisting of open reduction and internal fixation, we will be prepared to perform a hemiarthroplasty should the need arise intraoperatively. The principal circumstance that makes us opt for hemiarthroplasty in three-part fractures, even in cases in which the tuberosities are displaced less than 1 cm, is when the bone in the humeral head is too severely osteopenic to permit any sort of fixation (Fig. 17-5). These cases require osteotomy of the lesser tuberosity at the time of hemiarthroplasty.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


