Chapter 8. Immediate care and major incidents
Immediate management of multiple injuries
The management of a patient with multiple injuries depends upon an organized and disciplined approach. The most spectacular injury is seldom the most dangerous while the one that goes unseen can kill the patient. If the ‘ABC’ routine below is followed, life-threatening conditions will be dealt with first and undiagnosed injuries kept to a minimum.
Immediate action
A – Airway.
B – Bleeding.
C – Circulation.
Check the airway
An obstructed airway causes death most rapidly and must be dealt with first. Complete obstruction of the airway is easily recognized but partial obstruction causes a gradually increasing hypoxia which can go unnoticed until the partial pressure of oxygen ( PO 2) falls to critical levels and the patient loses consciousness. Always check the airway.
The airway can be obstructed by blood, vomit, broken teeth or dentures, soft tissue swelling around injuries to the neck or larynx, or facial fractures (Fig. 8.1). The first step in resuscitation is to check that the mouth and pharynx are clear (Fig. 8.2).
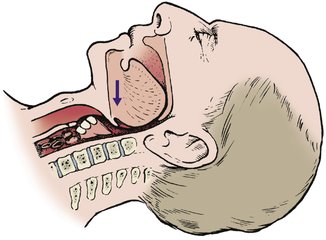 |
| Fig. 8.1 Obstruction of the airway. The tongue, broken dentures, blood, vomit or a fractured mandible can all obstruct the airway. |
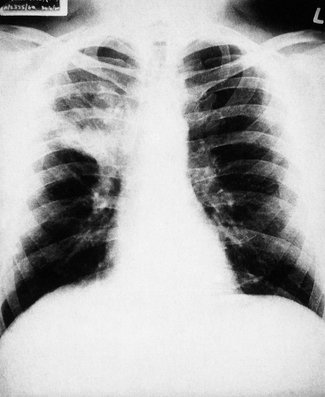 |
| Fig. 8.2 Consolidation of the right upper lobe after inhalation of a foreign body by an unconscious patient. |
Respiratory failure can also be caused by chest injuries such as a pneumothorax or flail chest, even if the airway is clear. Pain can also inhibit breathing, and respiratory failure can follow cervical spine fractures above C3 because the phrenic nerve (C3, 4, 5) is damaged, but this complication is so serious that the patients seldom reach hospital. Chest movement and respiratory rate should be checked regularly.
Endotracheal or nasotracheal intubation, or even tracheostomy may be needed to establish an airway.
Stop bleeding
Bleeding is best stopped by external pressure with a thumb or fist over the bleeding point, but a tourniquet may be needed to control bleeding from a limb. Whenever a tourniquet is used, the time of application must be recorded carefully and the tourniquet released after proper control of the haemorrhage has been achieved, or once every hour, to avoid gangrene.
If there is venous bleeding from a limb, lift the bleeding point above the level of the heart. This will stop the bleeding and improve blood pressure.
Restore blood volume
A large intravenous infusion line should be set up as soon as the airway is established and bleeding controlled. Entering a vein is difficult in the deeply shocked or hypovolaemic patient because the vessels will have collapsed. If the usual veins in the forearm cannot be entered, try the cephalic or external jugular. If these cannot be entered either, cut down onto a vein. The long saphenous vein at the ankle is convenient and is reliably found 3 cm above the tip of the medial malleolus and one-third of the way back from the anterior edge of the tibia (Fig. 8.3).
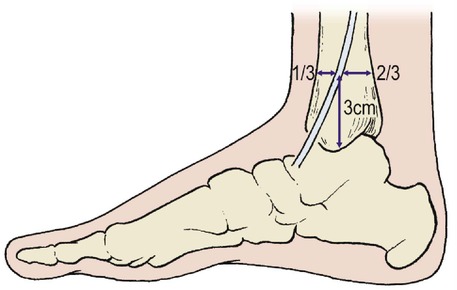 |
| Fig. 8.3 Site for saphenous cut-down. The long saphenous vein lies 3 cm above the medial malleolus, one-third of the way between the anterior and posterior surfaces of the tibia. |
In a well-organized accident department there will be enough people to do all these things at once while the patient’s clothes are removed – it is better to cut clothing off rather than pull it over limbs that may be fractured.
A skilled resuscitation team can establish an airway, arrest bleeding, remove the patient’s clothes and set up an intravenous line within minutes of the patient entering the resuscitation unit.
Monitoring and complete examination
When these steps have been taken, the resuscitation team is in control of the situation and less immediate problems can be dealt with.
When immediate action is complete:
1. Begin charts.
2. Examine the patient completely.
3. Record ECG.
4. Set up central venous pressure (CVP) line.
5. Check the patient again.
6. Notify appropriate specialists.
7. Grade injury.
Charts
Set up a record of the pulse rate, blood pressure, respiratory rate and neurological signs, including level of consciousness and pupil sizes, as soon as possible.
Complete examination
The entire patient should be inspected for wounds, including the back. If there is any possibility of a spinal injury the patient should be ‘log rolled’, until radiographs are available, to minimize the risk of displacing the fracture. The cervical spine should be protected at all times.
If this thorough inspection is not done very early, injuries will be missed. It is not only embarrassing but reprehensible to save the life of a patient and then find that he cannot work because of a malunited finger that needed only a few turns of adhesive strapping to achieve a perfect result.
Measure the wounds. Bruises and lacerations should be inspected, measured and recorded. Look particularly at the abdominal skin: bruising or imprints of clothing mean that there has been a violent blow to the abdomen and intra-abdominal bleeding should be suspected. Look also for signs of seat-belt bruising.
Examine every bone in the body




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
