CHAPTER 3 Imaging
Plain Radiographs
Basic science
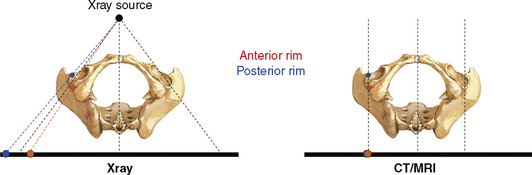
To understand the projected anatomy of the hip and the potential technical pitfalls related to it, it is essential to know the basic geometric radiographic principles. Conventional radiography is based on a point-shaped radiation source. In contrast with computed tomography scanning and magnetic resonance imaging, the image shows a distorted projection of the real anatomy. This conical projection implies that objects lying closer to the x-ray source necessarily will be projected more laterally (Figure 3-1).
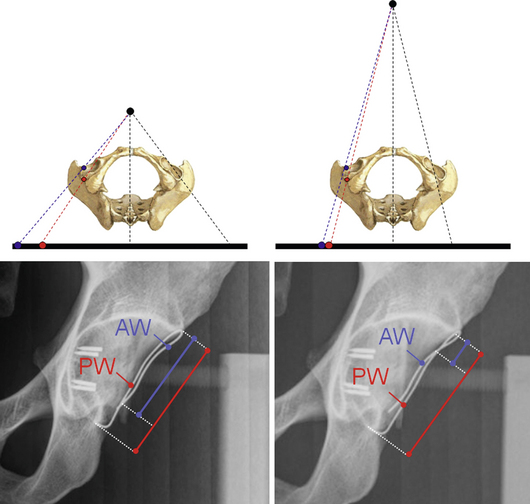
To obtain reproducible x-ray projections, it is mandatory that the film-focus distance is standardized. A radiograph with a very small film-focus distance can lead to a magnification of anatomic structures that are lying closer to the x-ray beam and vice versa (Figure 3-2).
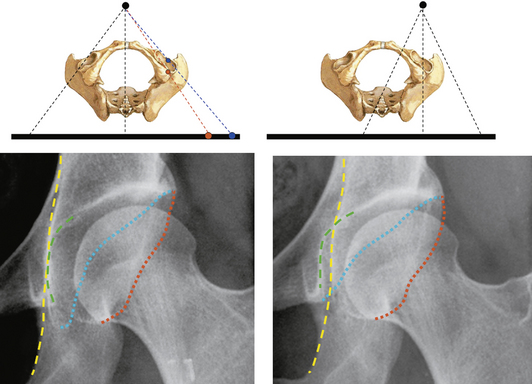
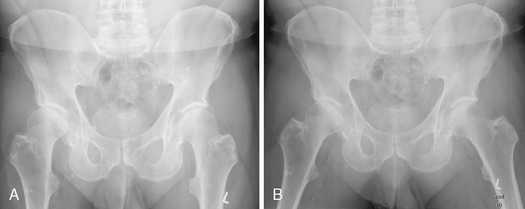
In addition, the proper centering of the x-ray beam is crucial. Two radiographs of the same patient taken with different beam centers can reveal a substantially different radiographic joint anatomy of the hip; this can typically be seen when radiographs of the entire pelvis are compared with radiographs of an individual hip (Figure 3-3).
Radiographic technique for specific projections
Anteroposterior Pelvic Radiograph
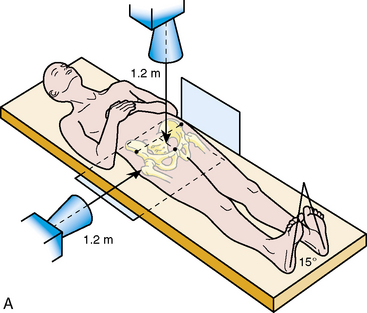
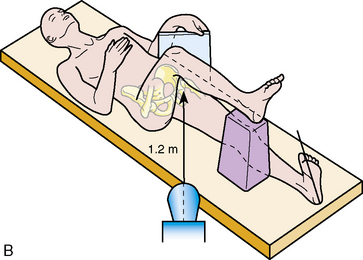
To correctly analyze hip joint morphology, an entire pelvic view—not only imaging of the affected hip—is mandatory. The AP pelvic radiograph is taken as a standard in our department, with the patient lying supine (Figure 3-4, A). This can be directly compared with intraoperative AP pelvic radiographs while the patient is under general anesthesia or with follow up radiographs during the early rehabilitation period. The legs have to be internally rotated to adjust for femoral antetorsion, and the film-focus distance should be 1.2 m. The central beam should be directed to the midpoint between the superior border of the symphysis and a line that connects both of the anterior superior iliac spines; these landmarks can easily and reproducibly be palpated by the radiology technician. It is extremely important for the correct interpretation of the radiographs that all radiographs are obtained with the same protocol.
Axial Cross-Table View of the Proximal Femur
The axial cross-table view of the proximal femur visualizes the anterior and posterior contour of the femoral head–neck junction, which cannot be seen on the AP pelvic radiograph. This image is taken with the patient in the supine position with the contralateral hip flexed and the ipsilateral leg internally rotated (Figure 3-4, B). Again, the film-focus distance is 1.2 m, and the central beam is directed to the inguinal fold with an angle of 45 degrees. As an alternative to this view, a Dunn-Rippstein view or a frog-leg lateral radiograph may be obtained.
False Profile
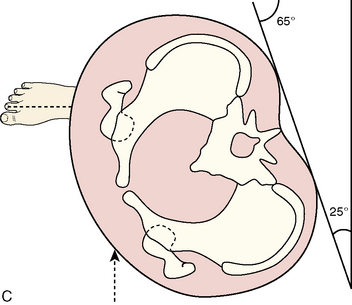
The false profile of the hip is taken with the patient standing (Figure 3-4, C). The index hip is in contact with the radiographic table, and the patient is rotated 25 degrees backward while the long axis of the foot remains parallel with the x-ray table. This view is used to quantify anterior acetabular coverage, the narrowing of the joint space posteroinferiorly or anterosuperiorly, and the decentration of the femoral head into the defect.
Abduction View
The abduction view is an analogous view to the AP pelvic radiograph, with the patient’s legs positioned in approximately 20 degrees of abduction and with the internal rotation of both legs. This view is used to simulate the appearance—particularly the congruency—of the hip after a planned hip reorientation osteotomy (Figure 3-5).
Radiographic parameters
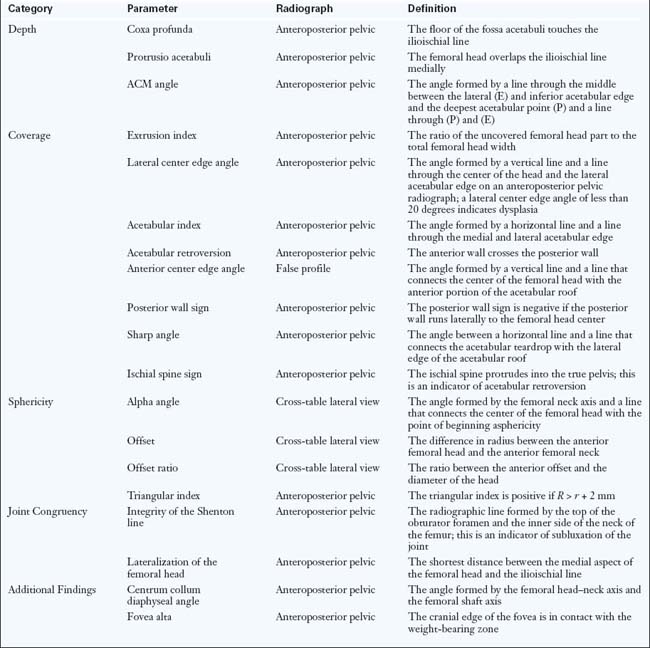
When evaluating conventional radiographs, the following features have to be evaluated: acetabular depth; acetabular coverage; the sphericity of the femoral head; joint incongruency; and additional findings (Table 3-1).
< div class='tao-gold-member'>
Related posts:
 Arthroscopic Labral Debridement
Arthroscopic Labral Debridement
 Supine Approach to Hip Arthroscopy
Supine Approach to Hip Arthroscopy
 Total Hip Arthroplasty in the Young Active Patient With Arthritis
Total Hip Arthroplasty in the Young Active Patient With Arthritis
 Surgical Hip Dislocation for Femoroacetabular impingement
Surgical Hip Dislocation for Femoroacetabular impingement
 Lateral Approach to Hip Arthroscopy
Lateral Approach to Hip Arthroscopy
 Computed Tomography, Ultrasound, and Imaging-Guided Injections of the Hip
Computed Tomography, Ultrasound, and Imaging-Guided Injections of the Hip
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


