Fig. 8.1
Normal anterior pelvic anatomy: standard MRI planes. (a) Coronal T1-weighted image through anterior pelvis. The rectus abdominis insertion (arrows) forms “mustache” along inferior margin of pubic bones (P). (b) Image just posterior to (a). Adductor longus tendons (arrows) are diverging low signal intensity triangles. Adductor brevis (ab) and pectineus (p) muscles lie laterally. (c) Transverse T2-weighted image shows rectus abdominis aponeurosis (arrows) as flat plate along anterior margin of pubic bones (P). (d) Image slightly inferior to (c). Unlike rectus abdominis insertions, adductor longus tendon origins (arrows) do not meet in midline
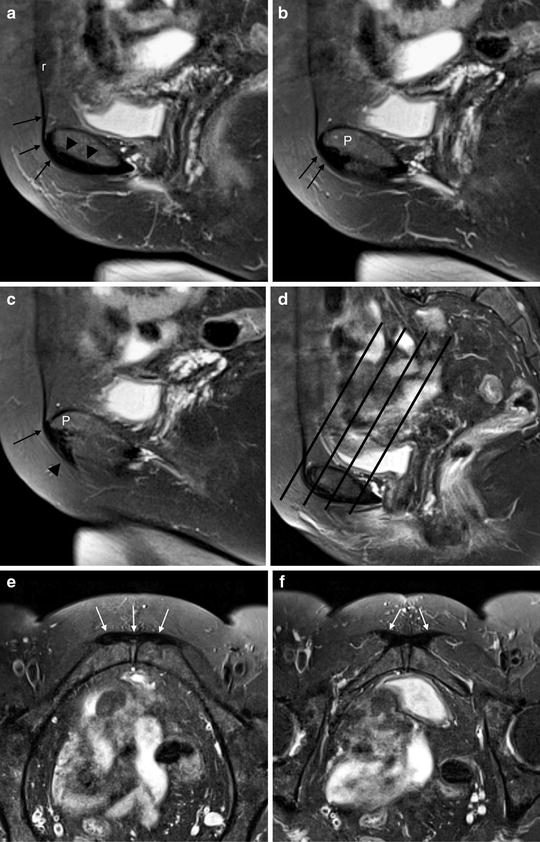
Fig. 8.2
Normal anterior pelvic anatomy: supplemental MRI planes. (a) Midline sagittal T2-weighted image. Rectus abdominis muscle (r), and tendon (arrows) blends with low signal intensity symphyseal joint capsule (arrowheads). (b) Sagittal image 3 mm lateral to (a). Rectus abdominis inserts (arrows) along inferior margin of pubic bone (P). (c) Sagittal image 3 mm lateral to (b). Triangular adductor longus tendon (arrowhead) originates from pubis (P). Note continuity of tendon with rectus abdominis tendon (arrow) forming common aponeurosis anterior to pubis. (d) Sagittal midline image with lines showing orientation of oblique transverse images. (e) Oblique transverse T2-weighted image showing rectus abdominis contribution (arrows) to normal aponeurotic plate. (f) Image just distal to (e). Proximal adductor longus tendons are triangular in shape (arrows)

Fig. 8.3
Normal adductor muscles. Oblique transverse T1-weighted image. Note relationships of proximal thigh muscle bellies. p pectineus, al adductor longus, ab adductor brevis, g gracilis
The two pubic bodies are joined in the midline by a non-synovial symphyseal joint [3], which together with the sacroiliac joints helps stabilize the pelvis, especially against the shear forces experienced during walking and running. A fibrous capsule completely encircles the joint and is normally low signal intensity on all MRI pulse sequences. The inferior capsule, referred to as the arcuate ligament, is the thickest portion [3]. The arcuate ligament merges with the aponeuroses of the gracilis and adductor longus [1]. A midline fibrocartilaginous disc sits between the opposing bone surfaces, which are covered by hyaline cartilage. Not uncommonly, however, a fluid-filled vertically oriented cleft will be visible on water-sensitive images centrally within this disc. Just off the midline, along the anterolateral surface of each pubic bone is a variable size tubercle. A secondary ossification along the anteromedial aspect of each pubic bone appears around adolescence, but these do not fuse to the rest of the pubic bones until age 20–25 years [2, 4].
The rectus abdominis muscles are enclosed in a sheath that may be visible as a thin low signal intensity structure on high resolution MRI or CT (Fig. 8.4). Superiorly the muscles have a broad origin on the ribs with the linea alba separating the two medial heads [1, 5]. Distally, separate medial and lateral muscle bellies are sometimes identifiable on cross-sectional images and these taper down to an aponeurosis cephalad to the pubic symphysis. On each side the aponeurosis wraps over the anterior edge of the pubic bone and then turns posteriorly where it is continuous with the proximal tendon of the adductor longus [2, 5, 6]. This common aponeurotic plate (sometimes referred to as the “prepubic aponeurotic complex” or PPAC) is anchored on the anteroinferior edge of the pubic symphysis, and can typically be seen in its entirety on parasagittal images approximately 3 mm from the midline (Fig. 8.2). The fibers of the aponeurosis blend with both the fibrocartilaginous disc and the pubic bone hyaline cartilage anteriorly [2]. The right and left aponeurotic plates also fuse together across the midline just above the adductor origin. On transverse images the normal aponeurosis is a continuous low signal intensity linear structure crossing the midline anterior to the pubis. On coronal images the lateral edge of the aponeurosis curves slightly downward; the appearance has been likened to a “mustache” underneath the pubic symphysis (Fig. 8.1).
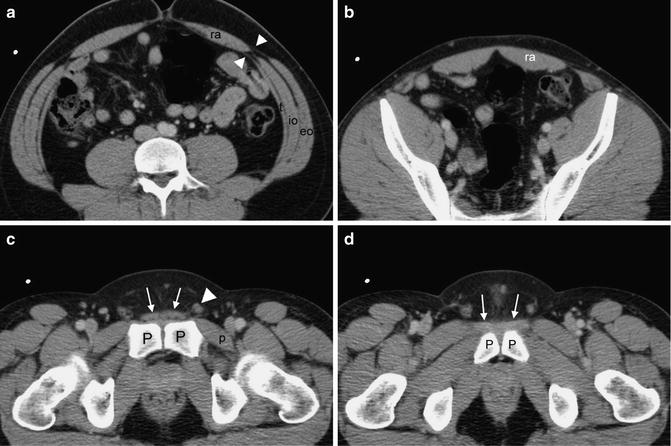
Fig. 8.4
Normal anterior abdominal muscles. (a) CT image through lower abdomen. Medial aponeuroses (arrowheads) of abdominal wall muscles—external oblique (eo), internal oblique (io), and transversus abdominis (t)—contribute to thin sheath surrounding rectus abdominis (ra) muscle. (b) Image through upper pelvis. Sheath around rectus abdominis (ra) muscle is now imperceptible. (c) Image through lower pelvis. Rectus abdominis contribution to aponeurosis (arrows) lies just anterior to pubic bones (P) and pubic symphyseal capsule. Note spermatic cord (arrowhead) along lateral margin of aponeurosis. Pectineus muscle (p) is deep to femoral vessels. (d) Image 2 mm distal to (c). Adductor longus tendons (arrows) originate from anterior pubis (P)
Along the inferolateral edges of the aponeuroses originate the two adductor longus tendons, which slightly diverge from each other as they extend caudally into their muscle bellies. The adductor longus tendons lie anterior to the other adductors. They can be recognized by their triangular shape in all imaging planes (Figs. 8.1 and 8.2) [5]. The proximal adductor longus tendon has a direct attachment to the medial pubic bone in addition to its contribution to the prepubic aponeurotic complex [2].
A common, fused tendinous origin of the gracilis and adductor brevis has been described [7]. The main origin of the adductor brevis is muscular, located posterior, lateral, and inferior to the adductor longus on the pubic bones; the adductor brevis frequently will also have some tendon fibers attaching to the symphysis [2]. The pectineus muscle lies along the lateral edge of the rectus abdominis muscle and it attaches to the superior pubic ramus posterior to the rectus abdominis. The pectineus muscle forms the floor of the femoral triangle and is visible deep to the femoral neurovascular bundle on cross-sectional images (Figs. 8.1 and 8.4) [5]. The adductor magnus muscle originates on the inferior ischiopubic ramus and ischial tuberosity, separate from the pubic body [1]. Other than the gracilis, which inserts on the tibia, the adductor muscles insert distally on the femur and work together to stabilize the pelvis during the swing phase of locomotion.
From superficial to deep, the external oblique, internal oblique, and transversalis abdominis muscles support the anterolateral abdominal wall. These muscles form a recognizable layered appearance on cross-sectional images near their attachments on the iliac wings (Fig. 8.4). The thick inferior edge of the external oblique aponeurosis forms the inguinal ligament [5]. Medially, the external oblique aponeurosis is thin, splitting to form the lateral border of the external inguinal ring, and then merging with the superficial rectus sheath. The internal oblique and transversalis fascia comprise the posterior abdominal wall and join with the deep rectus sheath (Fig. 8.4); a defect in the transversalis fascia corresponds to the internal inguinal ring [5]. The inguinal canal lies along the lateral border of the distal rectus abdominis muscle. In men the canal contains the spermatic cord; in women, the round ligament.
Acute Abdominal and Groin Injuries
Most acute sports injuries in the anterior abdominopelvic wall and groin are muscle strains (pulled muscles) due to sudden eccentric muscle activity. The imaging characteristics of these injuries are the same as the much more common muscle strains in the lower extremities [8]. Typically, strains involve the myotendinous junction or peripheral myofascial junction of one or more muscles (Fig. 8.5). High signal intensity edema and petechial hemorrhage will track along the muscle fibers resulting in a characteristic “feathery” appearance on water-sensitive MRI sequences [9]. Mild (grade 1) strains do not result in macroscopic fiber disruption. In grade 2 injuries, some but not all of the muscle and tendon fibers will be disrupted; a macroscopic hematoma may collect in the resultant gap, and be visible as a high signal intensity intramuscular mass on T1-weighted images (Fig. 8.6). Rarely, a severe injury can tear the entire muscle belly or myotendinous junction, a grade 3 injury [10].

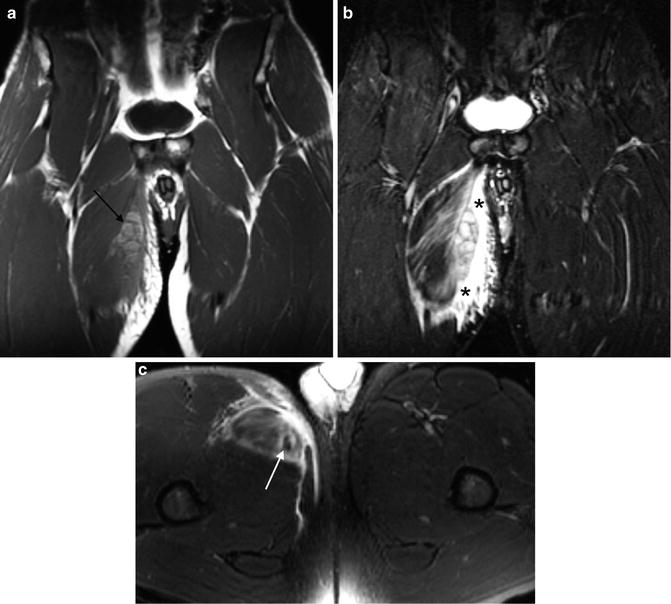
Fig. 8.5
Grade 1 adductor longus strain. (a) Coronal T1-weighted image appears normal. (b) Coronal STIR image shows “feathery” edema (arrow) tracking along the proximal myotendinous junction of adductor longus
Fig. 8.6
Grade 2 adductor longus strain (partial tear) in professional football linebacker. (a) Coronal T1-weighted image shows high signal intensity hematoma (arrow) in muscle. (b) Coronal STIR image demonstrates partly disrupted fibers (*) in addition to muscle edema. Compare to Fig. 8.5b. (c) Transverse T2-weighted image shows fascial and muscle edema surrounding central adductor longus tendon (arrow)
Groin muscle strains are more common than abdominal strains. The proximal myotendinous junction of the adductor longus is affected more frequently than the other adductors [5]. The deep surface of the rectus abdominis muscle is also susceptible to strains, especially in tennis and kicking sports, usually involving the muscle contralateral to the racket arm or dominant kicking leg [5]. In elite athletes, physiologic hypertrophy of the weak-side rectus abdominis can occur, which may predispose the muscle to injury (Fig. 8.7) [11].
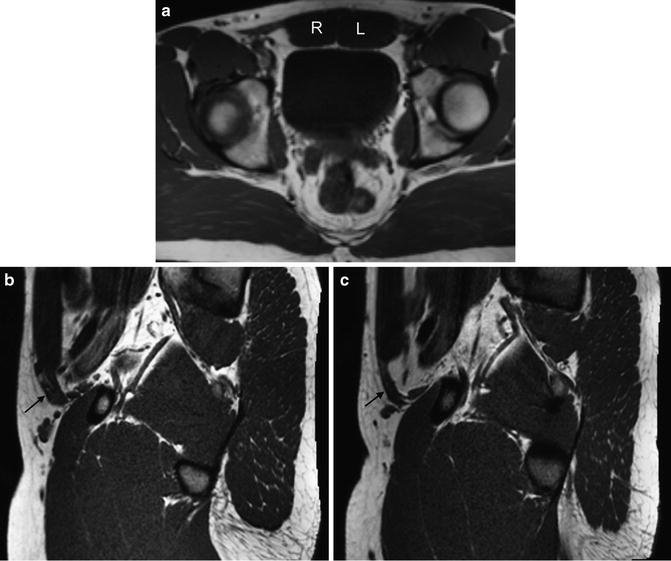
Fig. 8.7
Physiologic left-sided muscle hypertrophy in right-handed professional baseball pitcher. (a) Transverse T1-weighted image. Note increased size of left (L) rectus abdominis muscle compared to right (R). (b) and (c) Parasagittal images through the (b) left and (c) right abdominal walls. Note difference in size of the oblique muscles (arrows)
In younger patients, violent injuries can also avulse a tendon from bone, with or without a small fragment of the bone cortex (or apophysis in skeletally immature persons). In the anterior part of the pelvis, avulsions of the rectus femoris from the anteroinferior iliac spine and of the adductor longus from the medial pubis are the most frequent injuries [12]. The torn tendon will typically retract a variable distance towards its muscle belly, with a gap visible between the tendon end and its attachment point (Fig. 8.8). MRI is useful for determining the completeness of these injuries and the location of the avulsed tissue in cases where surgical repair is indicated. Traction injuries like avulsions tend to create much less marrow edema in the underlying bone compared to impaction and compression injuries [13]. Unlike the case for tendon tears that occur within the tendon substance, underlying tendinopathy is not a prerequisite for traumatic tendon avulsions from bone.

Fig. 8.8
Acute proximal adductor avulsions. Coronal STIR image. Adductor longus tendon (arrow) is torn from pubis and retracted distally. Muscular origin of adductor brevis (*) is also partly avulsed from bone
Chronic Athletic Pubalgia
Marrow edema in the anterior pubic bones, or a high signal intensity intraosseous line paralleling the pubic articular margin on water-sensitive sequences, is visible in greater than 90 % of athletes with groin pain in some series [14]. Previously, pubic marrow edema would often be ascribed to a primary bone “stress injury,” and there is data showing that the MRI finding does correspond to reparative new bone formation histologically, supporting the notion of a stress injury [15]. Now, however, most investigators consider these marrow changes as reactive and not primary [16]. Especially when it is asymmetric, pubic marrow edema should prompt a careful search for associated rectus abdominis and/or adductor longus injuries (Fig. 8.9). It is still not clear whether the bone marrow findings are simply a marker, or whether they represent a pain generator—or even the primary cause of pain—in patients with athletic pubalgia. Nevertheless, marrow edema by itself does not seem to be a strong prognosticator: in a cohort of Australian football players, preseason marrow edema was not associated with either groin pain or games missed in the subsequent season [17].
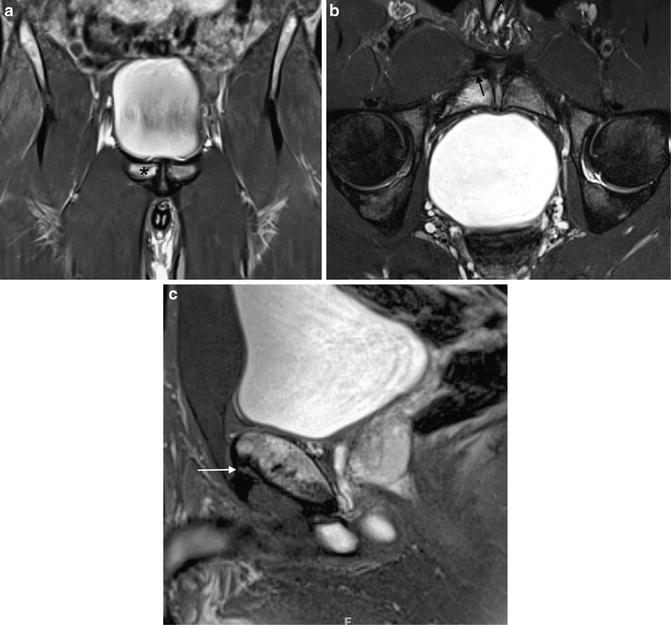
Fig. 8.9
Chronic athletic pubalgia. Treatment included adductor tendon release as well as pelvic floor repair. (a) Coronal STIR image. High signal intensity marrow edema is present in right pubic bone (*). (b) Oblique transverse T2-weighted image. Adductor longus tendon is partly torn from right pubic bone (arrow). Compare to Fig. 8.2f. (c) Sagittal image confirms injury at adductor longus tendon origin (arrow). Compare to Fig. 8.2c
The imaging hallmark of typical athletic pubalgia is injury to the common rectus abdominis–adductor longus aponeurosis [18, 19]. While retracted tears of the aponeurosis will be visible in the coronal plane (Fig. 8.10), nondisplaced avulsions may only be visible on oblique or sagittal images, which profile the anteroinferior margin of the pubis (Fig. 8.11). Bilateral aponeurotic injuries may separate the entire anterior aponeurotic plate from the pubis as a whole, crossing the midline (Fig. 8.12).

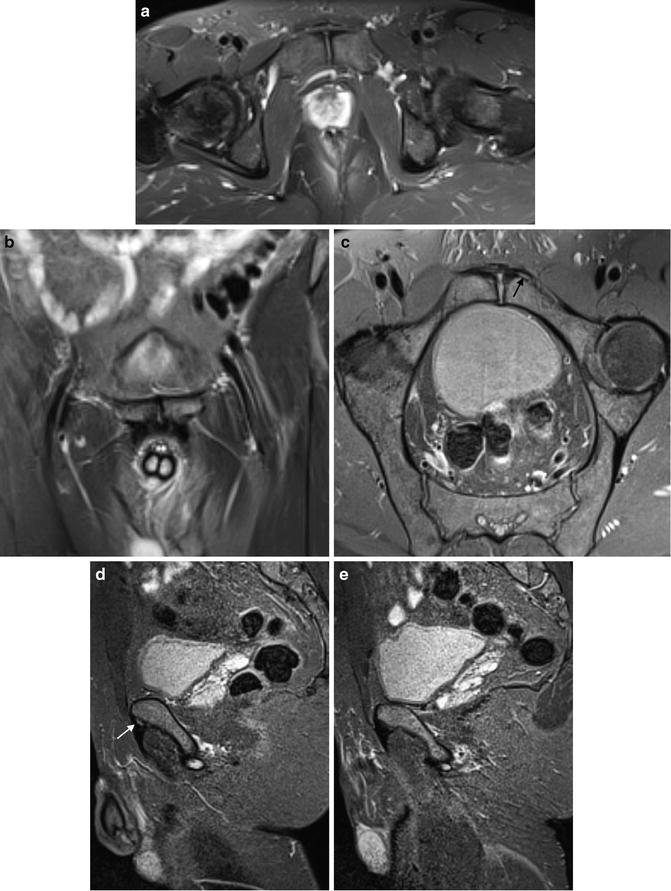
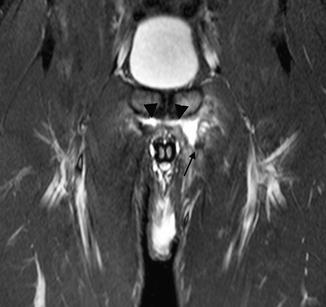
Fig. 8.10
Chronic athletic pubalgia. Coronal STIR image. Right rectus abdominis–adductor longus aponeurosis (arrow) is separated from pubic bone and retracted distally
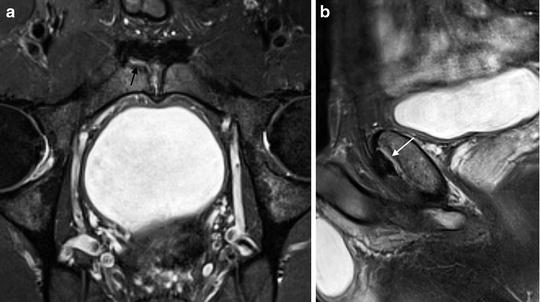
Fig. 8.11
Chronic athletic pubalgia. (a) Transverse and (b) coronal images appear normal. (c) Oblique transverse image shows subtle separation of rectus abdominis–adductor longus aponeurosis (arrow) from left pubic bone. (d) Sagittal image through left side confirms abnormality (arrow). (e) Sagittal image through normal right side for comparison
Fig. 8.12
Bilateral athletic pubalgia. Coronal STIR image shows entire aponeurotic plate (arrowheads) avulsed from both pubic bones and symphysis. On left, adductor longus tendon (arrow) is also torn and retracted distally
Depending on the surgical approach planned, it may be useful to determine whether the main injury is on the rectus abdominis or adductor side of the common aponeurosis [20], a distinction that is often difficult based on physical examination findings [18]. One useful imaging sign is a curved, high signal intensity line along the inferomedial corner of a pubic bone on a coronal water-sensitive image (Fig. 8.13), a finding that is not present in control subjects [21]. This “secondary cleft”—so called to distinguish it from the primary central cleft sometimes normally seen within the pubic symphysis disc—is a fairly reliable sign indicating a distal insertional tear of the rectus abdominis, especially when marrow edema is also present in the subjacent pubis (Fig. 8.14) [18]. Secondary clefts are continuous with the central symphyseal cleft, and anesthetic injections into the primary symphyseal cleft will fill a secondary cleft (Fig. 8.15), often resulting in pain relief [21]. When bilateral secondary clefts are present, rupture of the entire aponeurotic plate from the pubis is likely [20]. In addition to subjects with athletic pubalgia, some athletes with osteitis pubis will also have a secondary cleft on their MRI studies [1, 21]. It is unclear whether these patients have coexistent osteitis pubis and athletic pubalgia, or whether the secondary cleft sign is not specific for athletic pubalgia.

 Surgical Treatment of Sports Hernia: Laparoscopic Approach
The Role of Femoroacetabular Impingement in the Etiology of Athletic Pubalgia and Sports Hernias
Sports Hernia—Anatomy: What Is a Sports Hernia?
Hip Dysplasia
Sportsman’s Groin and the Inguinal Ligament Release Procedure
Surgical Treatment of Sports Hernia: Open Mesh Approach
Surgical Treatment of Sports Hernia: Laparoscopic Approach
The Role of Femoroacetabular Impingement in the Etiology of Athletic Pubalgia and Sports Hernias
Sports Hernia—Anatomy: What Is a Sports Hernia?
Hip Dysplasia
Sportsman’s Groin and the Inguinal Ligament Release Procedure
Surgical Treatment of Sports Hernia: Open Mesh Approach




Fig. 8.13
Athletic pubalgia with secondary cleft. Coronal STIR image shows very high signal intensity line (arrows) extending along inferior margin of right pubic bone
Related posts:
Surgical Treatment of Sports Hernia: Laparoscopic Approach
The Role of Femoroacetabular Impingement in the Etiology of Athletic Pubalgia and Sports Hernias
Sports Hernia—Anatomy: What Is a Sports Hernia?
Hip Dysplasia
Sportsman’s Groin and the Inguinal Ligament Release Procedure
Surgical Treatment of Sports Hernia: Open Mesh Approach
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
