Iliac Crest Bone Graft Harvesting
Sreeharsha V. Nandyala
Alejandro Marquez-Lara
Junyoung Ahn
Kern Singh
DEFINITION
The use of autogenous bone graft is considered by most surgeons to be the gold standard for achieving fusion in the spine.
Autogenous bone graft can be used at any spinal level, anterior or posterior.
The posterior ilium is most frequently harvested for nonstructural, cancellous bone graft.
Tricortical, structural bone grafts for cervical interbody fusions are typically harvested from the anterior ilium.
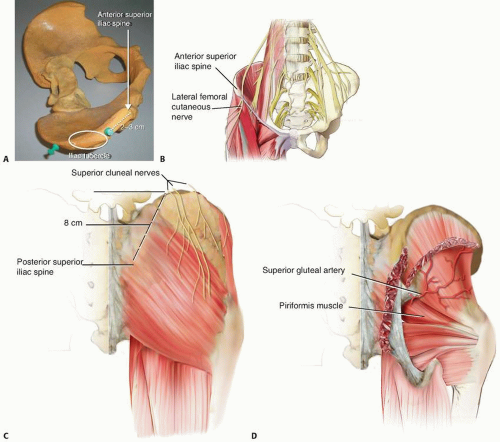 FIG 1 • A. Ideal anterior iliac crest bone graft is obtained 2 to 3 cm posterior to the ASIS. B. The lateral femoral cutaneous nerve generally traverses medial to the ASIS. C. The superior cluneal nerves cross the posterior iliac crest 8 cm anterior to the PSIS. D. The superior gluteal artery exits from the greater sciatic foramen. |
ANATOMY
Anterior ilium
The anterior ilium has a concave anterosuperior surface.
The anterior iliac crest is thickest (iliac tubercle) 2 to 3 cm posterior to the anterior superior iliac spine (ASIS) (FIG 1A).
The lateral femoral cutaneous nerve typically courses medial to the ASIS; however, it can infrequently cross lateral to the ASIS and be at risk for injury (FIG 1B).
Posterior ilium
The posterior iliac crest thickness ranges from 14 to 17 mm.
The superior cluneal nerve passes over the iliac crest 7 to 8 cm lateral to the posterior superior iliac spine (PSIS) and is at risk for injury with a lateral incision (FIG 1C).
The superior gluteal artery exits the pelvis from the greater sciatic notch and can be injured if bone harvesting approaches the sciatic notch (FIG 1D).
SURGICAL MANAGEMENT
Positioning
A roll or bump of towels or a blanket beneath the ipsilateral ischial tuberosity can facilitate access to the anterior iliac crest.
TECHNIQUES
▪ Surgical Approach
Anterior Iliac Crest
A skin incision is made parallel to the iliac crest and is centered over the iliac tubercle.
The incision is carried down to the fascia overlying the iliac crest. Subperiosteal dissection is then performed to expose the wing of the ilium. Care is taken to preserve the fascia so that it can be repaired, minimizing postoperative pain from the graft site. (TECH FIG 1).
The tensor fasciae latae, gluteus medius, and gluteus minimus originate from the lateral aspect of the ilium. These muscles are innervated by the superior gluteal nerve.
The abdominal muscles are also attached to the iliac crest and are segmentally innervated. The incision over the crest is, therefore, internervous and safe.
 TECH FIG 1 • The anterior iliac crest (arrow). |
Posterior Iliac Crest
The posterior superior iliac crest is often palpable under the skin dimple in the superomedial aspect of the gluteal region.
A vertical incision over the PSIS is made to minimize injury to the cluneal nerves.
An oblique or curved incision may be made over the posterior iliac crest. The cluneal nerves cross the iliac crest 7 to 12 cm anterolateral to the PSIS; therefore, the incision should be made medial to this cutaneous innervation.
The subcutaneous tissue is divided to the level of the iliac crest.
Using Bovie cautery, the iliac crest is incised.
The muscles are elevated subperiosteally from the posterolateral surface of the ilium.
The gluteus maximus, medius, and minimus originate from the lateral surface of the ilium. The superior gluteal nerve innervates the gluteus medius and minimus, and the inferior gluteal nerve innervates the gluteus maximus.
The paraspinal musculature is innervated segmentally.
Posterior Iliac Crest: Midline Skin Incision
A midline spine incision may be extended distally and the posterior iliac crest approached laterally under the skin and subcutaneous fat. This avoids a second skin incision.
The fascia overlying the PSIS is incised on the medial surface where it is more robust; this facilitates fascial closure upon completion of the bone graft harvesting.
The PSIS is exposed on its outer surface with the aid of electrocautery via a subperiosteal dissection.Related posts:
 Anterior Cervical Discectomy and Fusion with and without Instrumentation
Anterior Cervical Discectomy and Fusion with and without Instrumentation
 Cervical Osteotomies for Kyphosis
Cervical Osteotomies for Kyphosis
 Transforaminal and Posterior Lumbar Interbody Fusion
Transforaminal and Posterior Lumbar Interbody Fusion
 Percutaneous Pedicle Screw Fixation and Fusion for Trauma
Percutaneous Pedicle Screw Fixation and Fusion for Trauma
 Surgical Excision of Intradural Spinal Tumors
Surgical Excision of Intradural Spinal Tumors
 Pelvic Fixation for Neuromuscular Scoliosis
Pelvic Fixation for Neuromuscular Scoliosis

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


