Chapter 55 Hyperventilation Syndrome/Breathing Pattern Disorders
 Introduction
Introduction
Hyperventilation Syndrome/Breathing Pattern Disorders Defined
Hyperventilation syndrome/breathing pattern disorders (HVS/BPDs) are described as follows:
• Hyperventilation is a pattern of overbreathing in which the depth and rate exceed the metabolic needs of the body at that time. This is usually seen at 30 breaths/min or more.
• Breathlessness usually occurs at rest or with only mild exercise.
• Physical, environmental, or psychological stimuli override the automatic activity of the respiratory centers, which are tuned to maintain arterial carbon dioxide (PaCO2) levels within a narrow range.
• Although at any given time, the body’s carbon dioxide (CO2) production is set at a certain level, the exaggerated breathing depth and rate associated with HVS/ BPDs eliminates CO2 at a faster pace, resulting in arterial hypocapnia (low CO2 in blood).
• The arterial hydrogen ion (pH) (acid/alkaline balance) rises into the alkaline region, thus inducing respiratory alkalosis.1
As a direct result of HVS/BPDs, many patients present with multiple symptoms, some of which mimic serious disease. However, blood tests, electrocardiograms (ECGs), and thorough physical examinations may reveal nothing out of the ordinary. Up to 10% of patients in general internal medicine practice reportedly experience HVS/BPDs as their primary diagnosis.2 Many individuals with HVS/BPDs experience severe and genuinely distressing symptoms, and considerable medical expenses are incurred in excluding more serious pathology.
Gender
More females than males have HVS/BPDs, ranging from a ratio of 2:1 to 7:1. The peak age of incidence is 15 to 55 years, although other ages can be affected.2 Women may be more at risk because of hormonal influences, because progesterone stimulates respiratory rate, and in the luteal (postovulation/premenstrual) phase, CO2 levels drop on average 25%. Additional stress can then “increase ventilation at a time when CO2 levels are already low.”3 A case report linked progesterone (medroxyprogesterone) therapy as a cause of hyperventilation in a 52-year-old menopausal woman.4
Normal Breathing Pattern
To recognize HVS/BPDs, one must be aware of the characteristics of a normal breathing pattern.
• The breathing rate should be 10 to 14 breaths/min, moving 3 to 5 L of air per minute through the airways of the chest.
• During the active inhalation phase, air flows in through the nose where it is warmed, filtered, and humidified before being drawn into the lungs by the downward movement of the diaphragm and the outward movement of the abdominal wall and lower thoracic structures.
• The upper chest and accessory breathing muscles should remain relaxed.
• The expiratory phase is ideally effortless as the abdominal wall and lower intercostals relax downward and the diaphragm ascends back to its original domed position, aided by the elastic recoil of the lung.
• A relaxed pause at the end of exhalation releases the diaphragm briefly from the negative and positive pressures exerted across it during breathing.
• Under normal circumstances individuals are quite unaware of their breathing.
• Breathing rates and volumes increase or fluctuate in response to physical or emotional demands, but in normal subjects they return to relaxed low chest patterns after the stimuli ceases.
Benefits of Normal Respiratory Function
• Normal performance of the brain, organs, and tissues of the body
• Normal speech and human nonverbal expression (e.g., sighing)
• Fluid movement (lymph, blood)
• Spinal mobility through regular, mobilizing, thoracic cage movement
• Digestive function via rhythmic positive and negative pressure fluctuations, via normal diaphragmatic function
Any chronic alteration in breathing function automatically modifies these functions negatively.
The Carbon Dioxide–Oxygen Balancing Act
Chaitow et al10 addressed the misconception that oxygen is “good” and carbon dioxide is “bad” by stating:
Respiratory Homeostasis
Jennett5 described the delicate homeostatic balancing act in which pH and CO2 are key features:
Pathophysiology
Physiologic and Pathophysiologic Causes of Altered Patterns of Breathing
Hyperventilation can be an appropriate physiologic response to the body’s metabolic needs; for example, tachypnea (rapid breathing) or hyperpnea (increase in respiratory rate proportional to increase in metabolism) may result as the respiratory centers respond automatically and appropriately to rising CO2 production due to exercise or organic disease that may be creating acidosis. It is therefore important to exclude organic causes that diminish PaO2 or elevate PaCO2 levels.6
• Respiratory: asthma, chronic obstructive respiratory disease, pneumonia, pulmonary embolus, pneumothorax, and pleural effusion. A case of carbon monoxide poisoning presenting as HVS has been reported.7
• Cardiovascular: acute and chronic left heart failure, right heart failure, tachyarrhythmias
• Renal: nephrotic syndrome, acute and chronic kidney failure
• Endocrine: Diabetes with ketoacidosis, pregnancy
• Pharmaceutic: aspirin, caffeine, amphetamine, nicotine, progesterone therapy
BPDs may also emerge from a background of established pathology (e.g., asthma, cardiovascular disease, kidney failure, chronic pain). Even tumor infiltrates into brain respiratory centers and central chemoreceptors have caused hyperventilation.8 Where this is the case, the aim of this chapter is not to explore these states, since they are discussed elsewhere in this textbook.
Fluctuating blood glucose levels may trigger HVS/BPD symptoms in patients with high carbohydrate diets, which produce rapid rises followed by sharp falls to fasting levels or below.6,9
Chaitow et al10 noted that the following factors could lead to altered breathing patterns through pH shifts:
• Ketoacidosis promotes deeper, faster breathing because the breathing centers respond to the higher CO2 content.
• Diarrhea results in the loss of alkaline plasma bicarbonate ions, which if prolonged, leads to acidosis. This stimulates corrective overbreathing to remove CO2 (as carbonic acid [H2CO3]) and normalizes the pH.
• Excessive vomiting causes loss of hydrochloric acid, shifting the body toward alkalosis, slowing breathing to allow CO2 to build up and restore pH. Hypoventilation is the result.
Categorization of Causes
The reasons for an individual breathing inappropriately can derive directly from structural, biomechanical causes, such as a restricted thoracic spine, rib immobility, or shortness of key primary and accessory respiratory muscles.
Other catalysts that may affect breathing function include environmental factors (e.g., altitude, humidity).11
The etiology of HVS/BPD may involve combinations of the factors listed previously; however, in most instances, altered breathing patterns, whatever their origins, seem to be maintained by nothing more sinister than pure habit.6,12
The Carbon Dioxide–Hydrogen Ion Connection
• The acidity of the blood is determined mainly by CO2.
• CO2 is the end-product of aerobic metabolism, deriving mainly from the mitochondria. CO2 is odorless, heavier than air and, if inhaled in its pure form, causes suffocation.
• CO2 is present in the atmosphere at a concentration of around two-hundredths of 1%, and is harmless to humans but adequate to sustain plant life.
• Transportation of CO2 occurs from the tissues into the blood and then to the lungs for exhalation. The body converts CO2 to H2CO3, of which there is a perpetual surplus.
• The lungs exhale around 12,000 mEq of H2CO3 per day, compared with less than 100 mEq of fixed acids excreted by the kidneys. Normal range of end-tidal CO2 pressure is 35 to 45 mm Hg.13
• Any increase in bodily activity produces CO2, acidifying the blood, unless more CO2 is excreted and/or exhaled.
• It is therefore obvious that changes in breathing volume relative to CO2 production regulate the moment-to-moment concentration of pH of the bloodstream (longer term regulation of pH is shared with the kidneys).
• It is the concentration of CO2 in the blood, not oxygen, that is the major regulator of breathing drive.
• Higher CO2 levels immediately stimulate more breathing, apparently on the assumption that abundance of CO2 means oxygen-poor air is being breathed, breathing has stopped, or something else is happening that is an antecedent to suffocation.
Oxygen Delivery and Smooth Muscle Constriction
An exercising muscle is acid, hypercarbic, and hot, and it benefits from increased unloading of oxygen from its capillaries.11
The effect of pH on oxyhemoglobin dissociation is called the Bohr effect.
Psychology and Hyperventilation Syndrome/Breathing Pattern Disorders
On a psychological level, Bradley14 described a “cascade of symptoms” (see Figure 55-1) in which an original cause (emotional or physical) leads to tension and anxiety that results in hyperventilation, possibly an acute hyperventilation attack, which (with repetition) over time, results in anticipation, anxiety, and avoidance behaviors or phobias, or both.
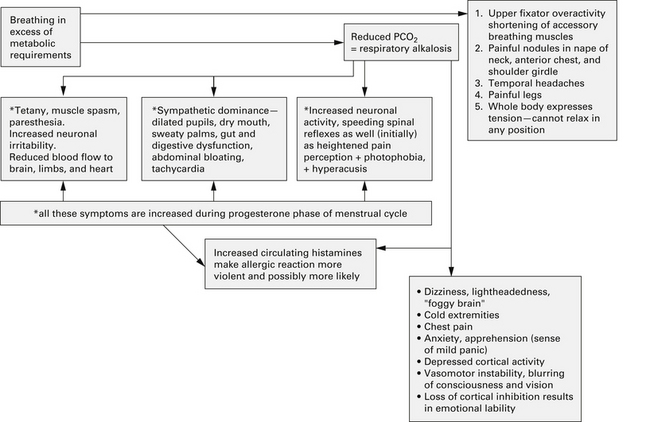
FIGURE 55-1 Negative health influences of a dysfunctional breathing pattern such as hyperventilation.
(From Chaitow L, Bradley D, Gilbert C. Multidisciplinary approaches to breathing pattern disorders. London: Churchill Livingstone, 2002:90.)
Chaitow et al10 described aspects of the influence of emotion on breathing15–17:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


