Chapter 174 Hypertension
 Diagnostic Summary
Diagnostic Summary General Considerations
General Considerations
Elevated blood pressure (BP) is a major risk factor for a heart attack or stroke. In fact, it is generally regarded as the most significant risk factor for stroke. More than 70 million Americans have high BP, including more than half (54.3%) of all Americans 65 to 74 years of age and almost three quarters (71.8%) of all American blacks in the same age group (Box 174-1). Additionally, 37% of U.S. adults have a blood pressure of 120 to 139/80 to 89 mm Hg, classified as prehypertension, which is associated not only with a greater likelihood of developing hypertension and cardiovascular disease, but also diabetes and cognitive impairment.1
Individuals with a normal diastolic pressure (<80 mm Hg) but elevated systolic pressure (>140 mm Hg), meaning an increased pulse pressure (>60 mm Hg), usually suffer from decreased compliance of the aorta (arteriosclerosis) and have a twofold increased risk of cardiovascular death as compared with those whose systolic pressure is normal (<120 mm Hg).1a Increased stroke volume due to aortic regurgitation, thyrotoxicosis, fever, and so on can also be a cause of increased pulse pressure.
High renin essential hypertensives make up approximately 15% of patients with essential hypertension. The elevation in renin (and associated high BP) is thought to be secondary to an increase in sympathetic nervous system activation.
Categorizing BP by renin level does not remain constant in a given patient. For example, a patient might be labeled as having low renin essential hypertension due to insulin resistance secondary to obesity. If the patient lost weight, regained insulin sensitivity, and yet the BP did not normalize, he or she would then be categorized as having normal or high renin essential hypertension. The categories based on renin level are primarily useful in identifying possible therapeutic interventions, as shown in Box 174-2.
BOX 174-2 Classifications of Hypertension
“White-Coat Hypertension”
White-coat hypertension has been defined as the persistent elevation of BP at the clinic or office only. Its prevalence may be as high as 20% to 45% of people diagnosed as hypertensive.1 It appears to be more frequent in women, older patients, and persons with Stage 1 hypertension. White-coat hypertension should not be confused with the white-coat effect, which signifies the difference in BP between the office and daytime ambulatory BP and occurs in patients with white-coat hypertension as well as in those with other causes of hypertension. The current conventional wisdom among naturopathic physicians is to treat white-coat hypertension as if it were essential hypertension. The reason for this stance is that current data suggest that the pressor response elicited mirrors real-life reactions to stress; that is, studies have suggested that white-coat hypertension is not an innocent phenomenon.2,3 In regard to the latter, a 21-year study comprising 536 men, those with a white-coat effect had a significantly higher rate of mortality than normotensive men and were nearly twice as likely to develop sustained hypertension.3
Ambulatory BP monitoring is a clinically useful tool for assessing suspected white-coat hypertension and cardiovascular risk.4 In patients with confirmed white-coat hypertension, drug treatment is usually not indicated; instead, treatment should consist of lifestyle and dietary modifications, weight reduction, regular exercise, smoking cessation, and correction of glucose and lipid abnormalities.1 In addition, semiannual or annual follow-up with ambulatory BP monitoring is advised.
Etiology
Essential hypertension is most likely the result of any number of factors that disrupt the regulation of arterial pressure and fluid volume. Vascular, hormonal, renal, and neurologic factors function in a complex interrelationship to maintain normal BP; disruption of any single facet disrupts the entire system and creates a cascading effect on regulatory mechanisms. Although genetic factors play a role, dietary, lifestyle, psychological, and environmental factors are the underlying causes in most cases of essential hypertension. Dietary factors include obesity; high sodium-to-potassium ratio; a low-fiber, high-sugar diet; high saturated fat and low omega-3 fatty acid intake; and a diet low in calcium, magnesium, and vitamin C. Important lifestyle factors that may cause high BP include stress, lack of exercise, and smoking. The dietary factor that has received the greatest attention is salt intake. Between 40% and 60% of hypertensive patients are salt sensitive. This factor is discussed below under “Therapeutic Considerations.”
Exposure to heavy metals like lead, mercury, cadmium, and arsenic may also be a significant factor in some patients. The kidneys are end-organ targets of heavy metals. Although studies of blood lead levels have not consistently shown an association, it is important to point out that blood lead levels reflect primarily acute exposure.5–7 Studies looking at bone lead, for example, have upheld that exposure to heavy metals is associated with an increased risk of hypertension.8 Specifically, the data suggest that lead has an acute effect on BP via either a recent exposure or cumulative dose. These associations were demonstrated in a cross-sectional analysis of 2001 to 2002 data from a community-based cohort in Baltimore, Maryland, of 964 men and women aged 50 to 70 years (40% African American, 55% white, 5% other race/ethnicity). Both blood lead and tibial lead were determined, along with systolic and diastolic BP. Blood lead was a strong and consistent predictor of both systolic and diastolic BP in models adjusted and not adjusted for race/ethnicity and socioeconomic status. Tibial lead was also associated with hypertension status before and after adjustment for race/ethnicity and socioeconomic status.8a
 Therapeutic Considerations
Therapeutic Considerations
Because more than 90% of patients with higher than optimal blood pressure have either prehypertension or Stage 1 hypertension, most can be brought under control through changes in diet and lifestyle.8b In fact, in head-to-head comparisons, many nondrug therapies such as diet, exercise, and relaxation therapies have proved superior to drugs in cases of prehypertension and Stage 1 hypertension. For Stage 2 hypertension, pharmacologic therapy may be necessary. Ideally, drug treatment should be used only until the dietary, lifestyle, and supplement strategies take hold. However, sometimes long-term drug therapy is required.
Current Pharmacotherapy of Hypertension
The use of a diuretic or any of the above-mentioned other drugs alone is referred to as a “step 1” therapy. Thiazide diuretics are still the most popular step 1 drugs but may soon be displaced by calcium channel blockers or ACE inhibitors. Beta blockers are not suitable step 1 drugs owing to their known side effects.9 Step 2 therapy comprises two medications, step 3 uses three, and step 4 approach involves four. Physicians are instructed to use single therapies before going on to the combinations, unless compelling indications are present, such as diabetes or heart failure.10
Overview of Dietary and Lifestyle Factors
In addition to the following discussion, several of these dietary and lifestyle factors are also discussed in Chapter 148, because the health of the artery is critical to maintaining normal BP.
Stress
Stress can be the causative factor of hypertension in many instances, although, as in other health conditions, it has more to do with the response to and processing of stress than with stress itself. Relaxation techniques such as deep breathing exercises, biofeedback, autogenics, transcendental meditation, yoga, progressive muscle relaxation, and hypnosis have all been shown to have some value in lowering BP.11 Although the effect is only modest, a stress reduction technique is a necessary component of a natural BP-lowering program.
One of the most powerful methods of producing less stress and more energy in the body is diaphragmatic breathing. Regular short exercise sessions of slow, regular diaphragmatic breathing have also been shown to lower BP in hypertensive individuals in several studies.12–14 One study in particular has shed light on the effect of breathing in hypertension.15 Volunteers with normal BP were taught shallow breathing. Measurement of the amount of sodium and potassium then excreted in their urine indicated that shallow breathing led to the retention of sodium in the body. It was suggested that this breathing pattern may play a causative role in some cases of hypertension owing to the retention of sodium. However, slow breathing (6 breaths per minute) has also been shown to improve oxygen saturation, exercise tolerance, and baroreflex sensitivity.16
RESPeRATE is a medical device that interactively guides the user toward slow, regular breathing by synchronizing voluntary respiration to musical tones. When used for 15 minutes daily, this device can lead to a significant reduction in BP. In one 8-week study, systolic BP was reduced 10.0 mm Hg and diastolic BP by 3.6 mm Hg, but not in the controls, and greater BP reduction was observed in those who demonstrated increased compliance with the device.17
Exercise
Epidemiologic studies have consistently demonstrated an inverse association between physical activity (or fitness) and hypertension. In addition to this evidence, clinical trials in hypertensive patients have clearly established that regular exercise is an effective treatment for high BP.18–22 Although it is generally thought that the greater the intensity of aerobic exercise, the greater the hypotensive effect, it has recently been shown that even mild to moderate aerobic exercise in as few as three exercise sessions per week with durations as short as 20 minutes produces a hypotensive effect.22 The degree of BP reduction from a regular exercise program is typically in the range of 5 to 10 mm Hg for both the systolic and diastolic readings. Patients with prehypertension and Stage 1 hypertension can typically bring their BP readings into the normal range with regular exercise.
Dietary Recommendations
The most important dietary goal for most patients with hypertension is achieving normal body weight. Obesity is the major dietary cause of hypertension, and achieving their ideal body weight is the most important therapeutic goal for most patients with any form of hypertension. From prehypertension all the way to chronic renal failure, weight loss can lead to complete elimination of the health issue, significant improvement, or at least a reduction in the number of prescriptions to be taken.23,24
Next to attaining ideal body weight, perhaps the most important dietary recommendation is to increase the proportion of plant foods in the diet. Vegetarians generally have lower BP levels and a lower incidence of hypertension and other cardiovascular diseases than nonvegetarians.25Although dietary levels of sodium do not differ significantly between these two groups, a vegetarian’s diet typically contains more potassium, complex carbohydrates, EFAs, fiber, calcium, magnesium, and vitamin C and less saturated fat and refined carbohydrates, all of which have a favorable influence on BP.
An increased intake of fruits and vegetables has been shown to lower BP.26 This effect may be due to increased antioxidant concentrations. Hypertensive patients have been shown to have increased oxidative stress, and antioxidants have been shown to block angiotensin II–induced increases in BP as well as to promote proper nitric oxide synthesis.27,28
The most useful foods for people with hypertension include the following:
• Nuts and seeds or their oils for their EFA content
• Cold-water fish (e.g., salmon, mackerel)
• Green leafy vegetables for their calcium and magnesium
• Whole grains and legumes for their fiber
• Foods rich in vitamin C, like broccoli and citrus fruits
• Foods rich in active flavonoids, including berries, cherries, grapes, and small red kidney beans
Celery is a particularly interesting recommendation for hypertension. It contains 3-n-butyl phthalide, a compound that has been found to lower BP. In animals, a small amount of this compound lowered BP by 12% to 14% and cholesterol by about 7%.29 The equivalent dose in humans can be supplied in about four to six ribs of celery. The research was prompted by the father of one of the researchers, who, after eating a quarter pound of celery daily for 1 week, observed that his BP had dropped from 158/96 to 118/82.
Garlic and onions are also important foods for lowering BP. Although most recent research has focused on the cholesterol-lowering properties of these vegetables, both have also been shown to lower BP in hypertension.30 In addition, commercial garlic supplements may be of benefit. The usual response to the use of garlic is fairly modest, roughly 8 to 11 mm Hg for the systolic and 5 to 8 mm Hg for the diastolic BP (see Chapters 62 and 63 for a full discussion and dosages).
“Dietary Approaches to Stop Hypertension”
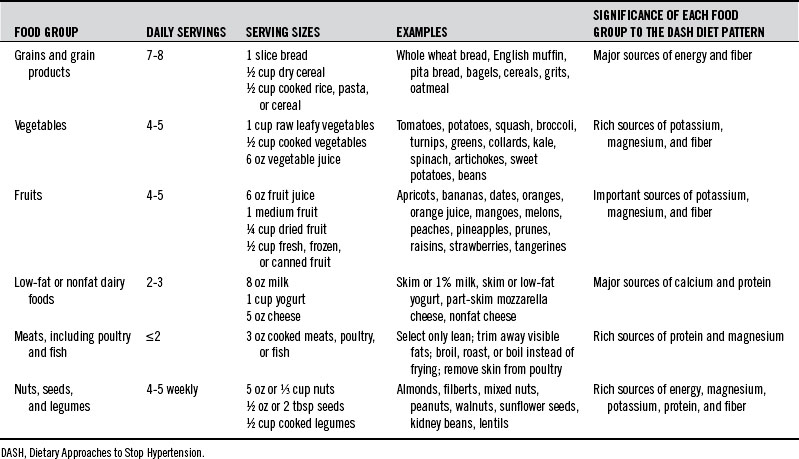
The first study showed that a diet rich in fruits, vegetables, and low-fat dairy products can reduce BP in the general population and people with hypertension.31 The original DASH diet did not require either sodium restriction or weight loss—the two traditional dietary tools to control BP—to be effective.32 The second study from the DASH research group found that coupling the original DASH diet with sodium restriction is more effective than either dietary manipulation alone.33 In the first trial, the DASH diet produced a net BP reduction of 11.4 and 5.5 mm Hg systolic and diastolic, respectively, in patients with hypertension. In the second trial, sodium intake was also quantified at a “higher” intake of 3300 mg/day; an “intermediate” intake of 2400 mg/day; and a “lower” intake of 1500 mg/day. Compared with the control diet, the DASH diet was associated with a significantly lower systolic BP at each sodium level. The DASH diet with the lower sodium level led to a mean systolic BP that was 7.1 mm Hg lower in participants without hypertension and 11.5 mm Hg lower in participants with hypertension. These results are clinically significant and indicate that a sodium intake below the recommended level of 2400 mg daily can significantly and quickly lower BP.
Table 174-1 lists a brief description of the components of the DASH eating plan on the basis of a 2000-calorie daily diet.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


