Chapter 40 Hydrotherapy*
 Introduction
Introduction History
History
Hippocrates used hydrotherapy extensively around 400 BC, and his writings concerning baths contain some of the earliest dictums on the therapeutic uses of water1:
In general it suits better with cases of pneumonia than in ardent fevers; for the bath soothes the pain in the side, chest and back; cuts the sputum, promotes expectoration, improves the respiration, and allays lassitude; for it soothes the joints and outer skin, and is diuretic, removes heaviness of the head, and moistens the nose.
Priessnitz’s philosophy of water cure was brought to the United States in the mid-nineteenth century. Joel Shew, a medical doctor from New York, studied with Priessnitz and returned to the United States to start a hydropathy institute based on his teachings. An associate of Shew’s, Russell Trall, MD, started his own hydrotherapy institute in Manhattan in the 1850s and later published the Hydropathic Encyclopedia. John Harvey Kellogg attended Trall’s institute, and in 1900 published Rational Hydrotherapy,2 in which he considered the physiologic and therapeutic effects of water, along with an extensive discussion of hydrotherapeutic techniques.
Benedict Lust, considered to be the father of naturopathy, was successfully treated by Father Kneipp and was charged with introducing the water cure to the United States. Lust successfully combined water cure with other nature cure modalities, establishing the foundation of naturopathic medicine. Henry Lindlahr, a wealthy U.S. banker suffering from diabetes, visited Kneipp after being told by his physicians that there was nothing they could do for him. He was put on a strict diet and daily regimen of cold water treatments. Once cured, he returned to the United States, completed medical training and opened a sanitarium in Chicago in 1906. He believed the vis medicatrix naturae was the true physician and wrote Nature Cure,3 the definitive guide to the philosophy and practice of nature cure medicine.
 Physiologic Effects of Water
Physiologic Effects of Water
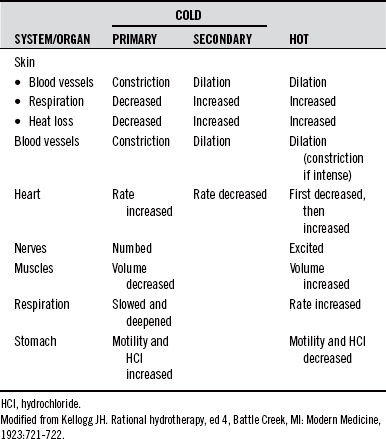
In general, hot relaxes and sedates, whereas cold stimulates, invigorates, and tonifies. However, very hot can stimulate and also be destructive, whereas prolonged cold can be depressive and destructive. A comparison of the effects of hot and cold on several body systems is given in Table 40-1.
Principles of Blood Movement with Hydrotherapy
Revulsive Effect
The revulsive effect provides a means of increasing the rate of BF through an organ or area of the body and is most effectively accomplished using contrast hydrotherapy: alternating hot and cold in the form of compresses, baths, showers, sprays, etc. Local contrast applications produce marked stimulation of local circulation. A 30-minute local contrast bath produces a 95% increase in local BF when the lower extremities alone are immersed. When all four extremities are immersed at the same time, there is a 100% increase in BF in the upper extremities and a 70% increase in the lower extremities.4
Several studies have researched the optimal treatment times for revulsive effects. Woodmansey et al5 found 6 minutes of hot application and 4 minutes of cold to be optimal for the British subjects he studied. Krussen6 found 4 minutes of hot and 1 minute of cold to be the best treatment protocol. Moor7 stated that 3 minutes of hot followed by 30 to 60 seconds of cold provided satisfactory clinical results. These variations create an inference that, due to variations in patients and locales, it is best for practitioners to determine their own ideals, based on their own observations of clinical results. Most importantly, the cold application needs to be long enough to produce vasoconstriction, which can occur in as short a period as 20 seconds. Additionally, the course of treatment should always end on cold to discourage congestion in the area.
Spinal Reflex Effect
A sufficiently intense local application of hot or cold not only affects the immediate skin area but also causes remote physiologic changes, mediated through spinal reflex arcs (see Moor7), thus providing a means of affecting a distant area of the body through a local application. These effects have been carefully observed over many years and have led to a mapping that correlates each surface area with a corresponding internal area and/or organ. Most texts on hydrotherapy contain such a diagram.2,7
Hewlett,8 Stewart,9 and Briscoe10 all noted changes in BF in the opposite arm and hand when one arm and hand were placed in hot or cold water. Poulton11 demonstrated that esophageal function could be influenced by irritation of the skin over the sternum. Bing and Tobiassen12 showed reflex relationships between the skin of the abdominal wall and the colon. They also demonstrated a reflex relationship between the lungs and the skin of the chest wall.
Fisher and Solomon13 stated: “externally applied heat not only decreases intestinal blood flow, but also diminishes intestinal motility and decreases acid secretion in the stomach, while cold has the opposite effect.” This is an example of a contrary effect, in which the reflex effect is the opposite of that observed in the local reflex skin area (i.e., local heat increases BF to the local skin, but decreases BF to the reflex organs).
Tables 40-2 to 40-4 show some of the observed reflex effects of hydrotherapeutic procedures.7
TABLE 40-2 Reflex Effects of Prolonged Heat
| APPLICATION LOCATION | EFFECT |
|---|---|
| One extremity | Vasodilation in contralateral extremity |
| Abdominal wall | Decreased intestinal blood flow, intestinal motility, and acid secretion |
| Pelvis | Relaxes pelvic muscles, dilates blood vessels, and increases menstrual flow |
| Precordium | Increases heart rate, decreases its force, and lowers blood pressure |
| Chest | Promotes ease of respiration and expectoration |
| Trunk | Relaxes ureters or bile ducts and relieves renal or gallbladder colic |
| Over kidney | Increases production of urine |
TABLE 40-3 Reflex Effects of Prolonged Cold
| APPLICATION LOCATION | EFFECT |
|---|---|
| Trunk of an artery | Contraction of the artery and its branches |
| Nose, back of neck | Contraction of the blood vessels of the feet and hands and nasal mucosa |
| Precordium (ice bag) | Slows the heart rate and increases its stroke volume |
| Abdomen | Increases intestinal blood flow, intestinal motility, and acid secretion |
| Pelvic area | Stimulates muscles of the pelvic organs |
| Thyroid gland | Contracts its blood vessels and decreases its function |
| Hands and scalp | Contraction of brain–blood vessels |
| Acutely inflamed areas | Vasoconstriction and relief of painful joints or bursae |
TABLE 40-4 Reflex Effects of Short Cold
| APPLICATION LOCATION | EFFECT |
|---|---|
| Local application of intense cold as brief as 30 s | General peripheral vasoconstriction |
| Face, hands, and head | Increase in mental alertness and activity |
| Precordial area | Increase in heart rate and stroke volume |
| Chest, with friction or percussion | Initial increase in respiratory rate, then slower, deeper respiration |
Collateral Circulation Effect
The collateral circulation effect may be considered a special case of the derivative effect.2 In general use, the derivative effect involves blood volume changes from one area of the body to another, as previously discussed. The collateral circulation effect, in contrast, more specifically considers the local circulatory effects on deep (rather than superficial) collateral branches of the same artery.
Considering the circulatory patterns of a large body part, such as the thigh, it is clear that both superficial and deep areas are supplied by the same artery. A hot application to this area dilates the surface vessels, drawing blood to the superficial areas and concurrently decreasing the BF to the deep areas. A cold application causes the opposite effect. Local compresses and fomentations are the most commonly used techniques to affect collateral circulatory changes.
Arterial Trunk Reflex
The arterial trunk reflex effect is a special case of the general reflex effect.2 Prolonged cold applied over the trunk of an artery produces contraction of the artery and its branches distal to the application. Prolonged hot applications have the opposite effect, producing dilatation in the distal arterial bed. For example, prolonged cold application over the femoral artery in the groin will decrease BF in a foot or ankle with an acute injury involving either internal or external hemorrhage. After the acute phase, prolonged hot applications can be used to increase circulation and speed healing of the injured part.
Local and Systemic Effects of Cold Applications
Cold applications are often prescribed for the relief of pain. Saeki5 found cold, but not hot, applications to be useful in the relief of prickly pain sensations experimentally induced in study subjects. Pain sensations were measured on the visual analog scale, and skin BF and skin conductance levels (SCL) were also measured. Cold applications decreased pain, BF, and SCL, whereas hot applications increased pain, BF, and SCL.
In 2002, a small (19 patients) study entitled “To Evaluate the Effect of Local Application of Ice on Duration and Severity of Acute Gouty Arthritis” was published.14 Treatment and control groups both received oral prednisone 30 mg tapered to 0 mg over 6 days and colchicine 0.6 mg daily. The treatment group received daily ice applications, whereas the control group did not. After 7 days, treatment group participants had a significant reduction in pain compared with the control group.
Cold water is very effective in lowering body temperature caused by fever due to illness or increased core temperature from exposure or exercise. Cold sponging has often been recommended for the reduction of fevers in children. Two articles published in 199715,16 compared the use of sponging to oral antipyretics. Both studies concluded that sponging was more effective than medication in the first 30 minutes, but after that, the antipyretic medications were more effective. This makes sense, because it takes time for the medications to be absorbed and circulate in the body, whereas the body responds immediately to the application of water to the skin. One of the primary precepts of naturopathic medicine is to work with the vis medicatrix naturae, and fever is one of the body’s responses to acute illness, assisting in the healing process. Lindlahr stated, “every so called acute disease is the result of a cleansing and healing effort of nature.”3 The benefit of sponging to reduce fever versus use of antipyretic medication is the ability to better control how much we reduce the fever, if at all.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


