Hip Resurfacing: Historical Overview
Michael Olsen
Emil H. Schemitsch
Total hip replacement (THR) is a common and proven procedure for patients suffering from end-stage hip disease requiring prosthetic intervention. Although there have been variations in the specific designs of THR systems over time, the basic principle of placing a stem in the medullary canal of the femur has remained unchanged. However, prior to the inception of total hip arthroplasty, the concept of replacing solely the diseased articular surfaces of the degenerative joint was explored. In fact, it was the early failure of these devices that led to the eventual establishment of total hip arthroplasty.
The History of Hip Resurfacing
In 1923, Dr. M.N. Smith-Peterson was the first to perform what would later become the basis for hip resurfacing arthroplasty. The initial design interposed a single, thin, temporary hemispherical shell between the femoral head and acetabulum. The aim was not to reconstruct the joint but rather regenerate the worn and damaged articular cartilage using the temporary shell and called this technique “mold arthroplasty.” The original shell was constructed from glass and inserted in an ankylosed hip in 1923 (1). Further material iterations of the device included celluloid, pyrex, and bakelite but the performance of these materials in situ was less than optimal often resulting in severe inflammatory reaction due to material wear debris in the joint. As a result, Smith-Peterson investigated new and emerging materials of the time including a new alloy of cobalt, chrome, and molybdenum, named Vitallium. Smith-Peterson first introduced a metal-mold arthroplasty from this material in 1938, coined the Smith-Peterson cup (Fig. 66.1).
The temporary shell design proved largely a failure, as regeneration of the degenerated articular surfaces was often incomplete and comprised of fibrous cartilage, and not articular cartilage as intended. The “mold” or “cup” arthroplasty concept spurred further designs based on the interposition of a shell between the femoral head and the acetabulum including the Luck cup in 1948. Designs like these gained modest interest and their experiences have been reported (2,3,4), however, they failed to gain widespread adoption.
Endeavoring to explore new materials in joint arthroplasty and learning from the tribulations of Smith-Peterson, Drs. Robert and Jean Judet introduced an acrylic femoral resurfacing implant in 1946 (5). The design of this implant incorporated a stem and was intended as a permanent implanted device. The shape of this prosthesis became the hallmark design for modern hip resurfacing femoral components (Fig. 66.2). This implant was poorly tolerated, however, eliciting an osteolytic reaction within the hip joint and surrounding tissue, and the acrylic material was soon discarded in favor of an alloy of cobalt and chromium (CoCr). This too was eventually abandoned in favor of the more predictable fixation of stemmed devices.
In the early 1950s, the concept of a double cup arthroplasty was introduced in which both the femur and acetabulum were fitted with articulating prostheses. John Charnley was the first to develop a total hip resurfacing system of this nature using Teflon (polytetrafluoroethylene) as the bearing material. Teflon was originally favored for its low coefficient of friction and its inert plastic properties and was described by Charnley (6) as “synthetic articular cartilage” in his initial paper discussing the use of the material in joint arthroplasty. The use of concentric shells of Teflon was short-lived with the overwhelming failure of these devices. At the time, Charnley (7) did not recognize the detrimental impact of the
bearing material and ascribed the failures to ischemic necrosis of the femoral head remnant citing “the most conservative feature of this design would be its undoing”.
bearing material and ascribed the failures to ischemic necrosis of the femoral head remnant citing “the most conservative feature of this design would be its undoing”.
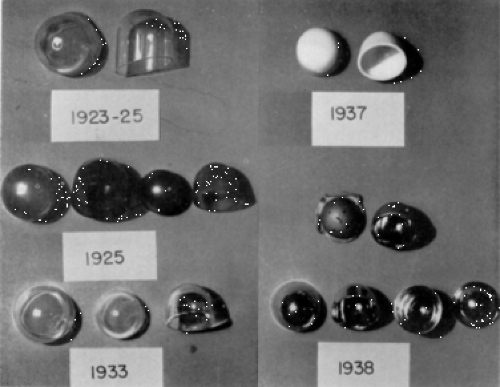 Figure 66.1. Evolution of the Smith-Petersen cup. 1923-glass; 1925-viscaloid; 1933-pyrex glass; 1937-bakelite; 1938-vitallium. (Reprinted with permission from Smith-Petersen MN. Evolution of mould arthroplasty of the hip joint. J Bone Joint Surg Br. 1948;30B(1):59–75.) |
 Figure 66.2. The Judet & Judet prosthesis. The prosthesis was a hemiarthroplasty design of acrylic material and was the hallmark design for modern hip resurfacing femoral components. (Reprinted with permission from Judet J, Judet R. The use of an artificial femoral head for arthroplasty of the hip joint. J Bone Joint Surg Br. 1950;32-B(2):166–173.) |
Charnley in turn used the Teflon material as an acetabular bearing surface in the earliest versions of his low-frictional torque total hip prostheses. Again, despite the promise of this material, osteolysis due to Teflon wear debris leads to catastrophic failure in many cases. Charnley (8) later conceded the role Teflon wear debris had to play in these failed devices and in 1962, Teflon as a bearing material would be altogether abandoned with the emergence of high-density polyethylene.
Building on the design of Judet & Judet, Charles Townley implanted a CoCr femoral component, fashioned with a slender alignment stem, articulating with a polyurethane acetabular cup in 1964 (9). The polyurethane cup ultimately demonstrated poor wear characteristics and was replaced by a CoCr acetabular component of which excellent long-term results have been published (10). An ultrahigh–molecular-weight polyethylene (UHMWPE) acetabular cup was later introduced but demonstrated inferior results to that of the Charnley THRs of the time (11).
The earliest use of a metal-on-metal bearing couple in hip replacement appears to be that of Philip Wiles in 1938 (12). With respect to hip resurfacing, it was Haboush (13) in 1951 who first implanted a metal-on-metal couple fixed with acrylic cement in two patients. However, it was not until 1968 when Müller and Boltzy (14) first published their results of a series of 18 hip resurfacings that the first metal-on-metal surface replacement was truly recognized. The original design consisted of a CoCr articulation with three small pads or “sliding bearings” fixed within the inner surface of the acetabular cup (Fig. 66.3). The sliding bearings consisted of Teflon or polyethylene. Despite “good early results,” Müller (15) abandoned the metal-on-metal articulation in 1968 for a curved stem metal-on-polyethylene prosthesis but later would question the appropriateness of the decision (16).
 Figure 66.3. Müller’s metal-on-metal hip resurfacing. The design consisted of an uncemented CoCr articulation with small pads of Teflon fixed to the inner surface of the acetabular cup. (Reprinted with permission from Amstutz HC. Hip Resurfacing: Principles, Indications, Technique and Results. Saunders Elsevier; 2008.) |
Remaining true to the principles established by Smith-Petersen, Gerard introduced a similar mold arthroplasty of CoCr for the hip in 1970. In addition to the press-fit mold for the femoral head, Gerard included a CoCr acetabular shell in his design and called the prosthesis a matching cup arthroplasty. In fact, the design utilized a Luck cup articulating in an Aufranc acetabular cup (17). The premise of the design was to encourage maximum motion within the metal interface, however, the acetabular cup was free to move against the prepared acetabulum and thus could theoretically accommodate for the extremes of motion. In an effort to reduce friction between the cups, a polyethylene version of the acetabular cup was introduced in 1972. This design was abandoned in 1975 due to accelerated wear and resulting bone resorption caused by the backside of the polyethylene cup articulating with the underlying reamed acetabulum (18).
Although the vast majority of hip resurfacing at the time was being performed in the western world, hip resurfacing also received considerable attention in Japan in the early 1970s. In 1972, Nishio at Kyushu University combined a Urist trident cementless acetabular cup with a Vitallium femoral head. Although at first the design consisted of a metal-on-metal articulation, the growing trend at the time produced a metal-on-polyethylene design that was implanted in 1975. Modest early results were reported in 1978 and Nishio et al. proposed hip resurfacing as a good adjunct to Charnley-type hip replacement in patients under 60 years of age (19). Nishio et al. (20) subsequently reported almost a 10% failure rate at short- (1 to 5 years
for metal-on-polyethylene implants) to midterm (5 to 9 years for metal-on-metal implants) follow-up.
for metal-on-polyethylene implants) to midterm (5 to 9 years for metal-on-metal implants) follow-up.
Table 66.1 Historical Evolution of Hip Resurfacing Arthroplasty: First and Second Generations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In retrospect, the failure of early hip resurfacing was the consequence of unproven material selection, metallurgical and manufacturing limitations of the time as well as unrefined surgical technique and instrumentation. In addition, crude implant design and a lack of solid implant fixation at the bone–implant interface was to blame for many of the failures of these first-generation devices. Improved implant materials coupled with better fixation methods became the major focus of future hip resurfacing designs (Table 66.1).
Hip Resurfacing Revisited
What was dubbed as the second generation of hip resurfacing emerged in the early to mid 1970s (Fig. 66.4). This was a time when THR was flourishing and limited, yet guarded, interest in hip resurfacing remained. This generation of hip resurfacing prostheses incorporated new bearing materials and refined surgical techniques that again breathed life into a bone-conserving method of hip joint replacement. The concept of cementing components to obtain rigid initial fixation became prominent and looked to eliminate many of the problems previously encountered with free-fixation or cementless designs. During this time, numerous surgeon designers introduced surface replacement systems employing a bearing couple of metal or ceramic articulating with polyethylene.
In 1971, Trentani in Italy and Furuya in Japan independently carried out the first cemented double cup arthroplasty. Trentani along with Paltrinieri developed a hip resurfacing comprises a collared stainless steel femoral head articulating with a UHMWPE acetabular cup (Fig. 66.5). The initial experience with the device was reported by Trentani and Vaccarino in 1978 comprising 70 patients where there was a 12% failure rate at a follow-up of 2 to 6 years (21). All failures occurred on the femoral side, either owing to femoral neck fracture or femoral component loosening, and it was noted that there were no signs of wear of the failed components.
Furuya’s design and findings were in contrast to that of Trentani. Furuya’s design mated a stainless steel acetabular cup with a high-density polyethylene femoral head, and following the first 13 hips performed with this prosthesis, at a length of 3 to 6 years, they demonstrated a 58% revision rate (22). There was one femoral neck fracture second to osteonecrosis while the remaining six failures occurred due to loosening of the cemented acetabular component. The failures were mainly attributed to patient selection citing the deleterious effect of the high degree of acetabular dysplasia exhibited by the patients with failed implants. At the time, authors like Trentani and Furuya, and those to follow, were unaware of the detrimental role polyethylene wear debris assumed in the failure of these devices.
At the London Hospital in 1972, Freeman first implanted a cemented double cup arthroplasty designed in the biomechanics unit of Imperial College. Aptly, the device was named
the Imperial College London Hospital (ICLH) hip resurfacing. Similar to Furuya, the prosthesis mated a CoCr acetabular cup with a high-density polyethylene femoral head. The initial experience with 16 such configurations implanted between May 1972 and April 1974 was reported at the British Orthopaedic Association meeting in 1974 (23). Four hips required conversion to a Charnley THR, all failing on the femoral side due to mechanical error. The implant design was revised in April 1974 to position a CoCr femoral head articulating with a high-density polyethylene cup and the subsequent 222 hips were detailed in 1983 (24). At a follow-up of 2 to 6 years, 21% (43/204) had failed, the majority of which were due to aseptic loosening. In reflecting on these results, Freeman asserted the theoretical advantages of hip resurfacing but tempered his support questioning the clinical merit of the procedure.
the Imperial College London Hospital (ICLH) hip resurfacing. Similar to Furuya, the prosthesis mated a CoCr acetabular cup with a high-density polyethylene femoral head. The initial experience with 16 such configurations implanted between May 1972 and April 1974 was reported at the British Orthopaedic Association meeting in 1974 (23). Four hips required conversion to a Charnley THR, all failing on the femoral side due to mechanical error. The implant design was revised in April 1974 to position a CoCr femoral head articulating with a high-density polyethylene cup and the subsequent 222 hips were detailed in 1983 (24). At a follow-up of 2 to 6 years, 21% (43/204) had failed, the majority of which were due to aseptic loosening. In reflecting on these results, Freeman asserted the theoretical advantages of hip resurfacing but tempered his support questioning the clinical merit of the procedure.
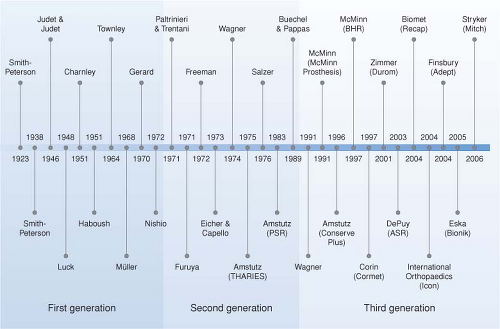 Figure 66.4. Timeline depicting the evolution of hip resurfacing. |
 Figure 66.5. The first cemented double cup arthroplasty by Paltrinieri and Trentani. (Reprinted with permission from Amstutz HC. Hip Resurfacing: Principles, Indications, Technique and Results. Saunders Elsevier; 2008.) |
Eicher first introduced the Indiana Conservative Hip (ICH) in 1973 and the initial results with the device were reported in 1978 by Capello et al. (25). Their design was in keeping with the cemented double cups of the time, mating a hemispherical CoCr alloy head against an eccentric UHMWPE cup. Eicher implanted 34 first-iteration ICH implants between 1973 and 1975 of which six suffered a femoral neck fracture and eight were revised for acetabular loosening (25). Shifting practice to the University of Indiana in 1975, the design was modified to include a medial cutout of the acetabular shell and a thinner-walled femoral
component. Over a 5-year period between 1975 and 1980, Capello implanted 116 ICHs in 96 patients. With a follow-up period of 2 to 7 years, he reported 17 failures overall (14.6%) with revision for loosening of the acetabular component, femoral component, or both occurring in 13 of 17 cases (26).
component. Over a 5-year period between 1975 and 1980, Capello implanted 116 ICHs in 96 patients. With a follow-up period of 2 to 7 years, he reported 17 failures overall (14.6%) with revision for loosening of the acetabular component, femoral component, or both occurring in 13 of 17 cases (26).
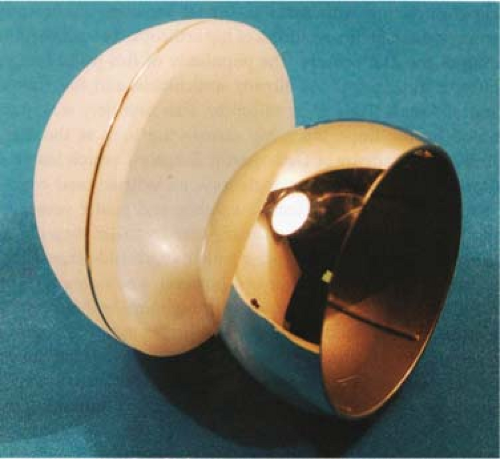 Figure 66.6. Original surface replacement by Heinz Wagner in 1974. The design employed both metal-(shown) and ceramic-on-polyethylene versions. This design was the first to employ a central aperture at the dome apex of the femoral component. (Reprinted with permission from Amstutz HC. Hip Resurfacing: Principles, Indications, Technique and Results. Saunders Elsevier; 2008.) |
While Freeman was reporting his first results with cemented metal-on-polyethylene hip resurfacing in London in 1974, Heinz Wagner had begun implanting his version of a hip surface replacement in Germany. However, Wagner’s design at the time was more in keeping with Eicher’s than Freeman’s. Not only did Wagner place a CoCr alloy head against a thin cemented high-density polyethylene cup, but he also introduced a ceramic head version as well (Fig. 66.6). This design was the first to employ a central aperture at the dome apex of the femoral component through which “air, blood, fatty marrow, and excess cement” could be extruded at the time of implantation. His initial experience of 426 hip resurfacings was reported upon in 1978 where he described the findings of 372 metal-on-polyethylene, 40 ceramic-on-polyethylene, and 14 ceramic hemiarthroplasties (27). With a follow-up of 6 months to nearly 4 years, six revisions were reported, all of which were the result of aseptic femoral and/or acetabular implant loosening.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


