7
HIP
Abby L. Cheng and Heidi Prather
INTRODUCTION
In the past our understanding of the hip joint, its function, and its acquisition of dysfunction was limited by the availability of only static imaging studies. Hip arthroscopy has expanded our knowledge of the cartilaginous and bony structural changes in the hip that imaging had not clearly shown. We have a better understanding of dysfunction related to structural changes that occur prior to the onset of arthritis, but we are also learning that correction of the structural changes does not always guarantee a correction of dysfunction and pain (1). This concept is particularly important when evaluating and treating young athletes because they often present with hip-related pain early in the disease course and are limited in their ability to participate in sports. We need to know how to manage this population appropriately in order to treat painful dysfunction and prevent future cartilaginous injury and adaptive movement changes that develop as a response to pain.
Now our understanding of the hip is further enhanced by three-dimensional modeling imaging with CT and MRI, which detail structural relationships, in addition to laboratory-based studies that are elucidating real-time movement relationships (2). There is emerging evidence of hip dysfunction patterns that are sex-related (3). As a result, there is an increasing awareness of a need to fill these knowledge gaps regarding the hip disorders and how they are related to each sex.
Evaluation of hip pain can be difficult because the referral pattern of hip pain is variable and overlaps in distribution with painful disorders of the lumbar spine and pelvic girdle. Furthermore, lumbar spine, pelvic girdle, and hip disorders coexist, and as a result pain may not be related to just one entity. Often the first step in coming to a hip-related diagnosis is to determine whether pain is caused by an intra-articular structural disorder (i.e., affecting the cartilage or labrum inside the hip joint) or extra-articular structural or movement disorder (i.e., affecting bone or soft tissue outside the joint capsule). This chapter refers to these concepts of differential diagnosis to review and describe hip disorders as they relate to sex, movement patterns, prearthritic conditions, hip osteoarthritis (OA), extra-articular soft tissue pathology, bone disorders, and other lumbopelvic pain conditions that are affected by hip motion.
NORMAL STRUCTURAL DIFFERENCES
Bony Differences
In addition to sex differences in pelvic girdle structure (discussed in Chapter 6), there are also sex-based differences in femur and acetabular anatomy (see Figure 7.1). Recognizing these differences is important in order to accurately define the continuum of normal versus aberrant bony hip structure.
Proximal Femur
The femoral head is often aspherical, and variations in femoral head shape can contribute to incongruent force and weight distribution across the joint. There are several radiographic measures designed to describe the femoral head shape and its relation to the acetabulum.
First, the alpha angle characterizes the “bulkiness” of the femoral head-neck junction. Larger alpha angles describe greater bulk of the proximal femoral neck (see Figure 7.2). The value for the “normal” alpha angle is still debated for two reasons: (a) the alpha angle of a given hip varies based on the plane being examined (i.e., on different radiographic views and different cuts on CT and MR imaging), and (b) for any given “normal” cutoff, abnormal proximal femur anatomy does not correlate one-to-one with symptomatic hip pain. Currently an angle above 60° in both sexes is most commonly considered to be abnormal (4). However, several studies have shown that alpha angles are consistently larger in males than females, both in adolescents and adults (5–7). This sex difference in alpha angle suggests that in order to have the highest accuracy in diagnosing abnormal hip morphology, it may be necessary to define different reference angles for each sex. At this time, there is no expert consensus on this aspect of description by sex. Further research is needed to better quantify appropriate angles to be used as cutoff points to discriminate between the range of normal and aberrant measurements.

FIGURE 7.1: Sex differences of hip anatomy. (A) There are sex differences in femur and acetabular bony anatomy. (B) Because females have wider pelvises, they have longer gluteus medius muscles and must generate more torque across the hip joint in order to maintain a level pelvis.
There are other radiographic measures also used to characterize proximal femur anatomy, but data on sex differences for these measures are less robust. The measures include femoral version, femoral head-neck offset, and femoral offset (see Figures 7.3–7.5 for descriptions of how these measurements are made). At this time in adults, there are mixed data regarding whether there is a sex difference in femoral version (2,8–10), and for femoral head-neck offset it seems there is no sex difference (5). However, for femoral offset males do have a significantly greater mean value than females (55 mm vs. 48 mm, respectively) (10). During adolescence, males also develop a proportionately greater femoral neck width, which provides increased structural integrity compared to females (11).
Lastly, the femoral head can be classified as spherical or aspherical in shape (12). While no studies have specifically evaluated for sex differences in sphericity in normal hips, there is disproportionate sex-specific representation of conditions manifesting as femoral head asphericity such as Legg-Calvé-Perthes disease (LCPD) and slipped capital femoral epiphysis (SCFE). These conditions will be discussed later in the chapter.

FIGURE 7.2: Alpha angle. The alpha angle describes the “bulkiness” of the femoral head-neck junction. It is the angle between (a) a line drawn along the longitudinal axis of the femoral neck and (b) the point along the femoral head-neck contour that first exceeds the radius of the femoral head.
Source: From Ref. (12). Clohisy JC, Carlisle JC, Beaule PE, et al. A systematic approach to the plain radiographic evaluation of the young adult hip. J Bone Joint Surg Am. 2008;90(Supp 4):47–66.
Acetabulum
Radiographic measures describing acetabular anatomy include acetabular version, center-edge angle (CEA), and Tönnis angle.
Acetabular version describes the anterior/posterior orientation of the opening of the acetabulum. As depicted in Figure 7.6, it is measured on an axial image and is the angle between a line perpendicular to the plane of the ischial tuberosities and a line connecting the anterior and posterior margins of the bony acetabulum. Acetabular anteversion refers to angles greater than 0°, and retroversion is defined as a version angle less than 0°. Females tend to have greater acetabular anteversion angles than males (mean/standard deviation 23° ± 10° versus 18° ± 9°, respectively) (10), and acetabular retroversion is more common in males (13).
The lateral CEA describes how much coverage the acetabulum provides over the femoral head. Too much acetabular coverage is a component of femoroacetabular impingement (FAI), and too little coverage is a component of hip dysplasia. Lateral CEA is measured on an anteroposterior (AP) pelvic radiograph and, as shown in Figure 7.7, is defined as the angle between a vertical line drawn through the center of the femoral head and a line connecting the center of the femoral head to the outer edge of the acetabular roof. Historically normal lateral CEA values have been accepted as 25° to 39° for both genders (12,14), and in more recent literature the measurement for the cutoff point for sex-specific normal lateral CEA values is conflicting (2,10,15–17). However, there are sex differences in impingement and dysplasia, and these are discussed in their respective sections later in the chapter.
Finally, acetabular inclination described by the Tönnis angle is a measure of the vertical tilt of the socket opening. As shown in Figure 7.8, it is calculated from an AP radiograph and is the angle between a horizontal line that crosses through the inferior aspect of the acetabular sourcil (i.e., the sclerotic weight-bearing aspect of the socket) and a line connecting the medial and lateral aspects of the acetabular sourcil. A normal angle is 0° to 10°, and there are no documented sex differences for this reference range (12).
Sex differences in normal acetabular structure evolve from childhood through adolescence. During adolescence, acetabular development occurs earlier in females, but males ultimately develop increased articular surface area compared to females (18). Anthropologic literature has also described variations in the shape of the inner surface of the acetabular socket. Some of these variations are unevenly represented between genders, and since bone structure is affected by its loading environment, it is possible that differences in acetabular shape are at least in part due to sex differences in movement patterns (19).
Range of Motion
Because of the differences in bony structure, it is logical to suspect that normal hip range of motion (ROM) would also be different between the sexes. In a study by Nakahara et al., evaluation of three-dimensional reconstructions of pelvic CT scans in elderly people without hip pain supports this hypothesis. Based on bony endpoints, females had greater maximum hip flexion and internal rotation at 90° of hip flexion, whereas males had greater maximum hip extension and external rotation at 90° of hip flexion (2). More studies are needed to support this finding in other populations (Table 7.1).

FIGURE 7.3: Femoral version. (A) Femoral version is defined as the angular difference between the femoral neck axis and the transcondylar axis of the knee. It is measured by superimposing axial CT cuts of both the femoral neck and the transcondylar axis to calculate the angle between the two. (B) Femoral version describes the “twisting” between the femoral neck and the femoral condyles. It affects rotation of the distal leg.
(A) Source: From Ref. (9). Koerner P, Patel NM, Yoon RS, et al. Femoral version of the general population: does “normal” vary by gender or ethnicity? J Orthop Trauma. 2013;27(6):308–311. (B) Source: Adapted from Ref. (127). Wilmerding V, Krasnow D. Turnout for Dancers: Hip Anatomy and Factors Affecting Turnout. Education and Media Committees of the International Association for Dance Medicine and Science (IADMS). 2011. www.iadms.org/?323. February 21, 2016.

FIGURE 7.4: Femoral head-neck offset. The femoral head-neck offset describes the taper of the femoral neck. It is the perpendicular distance between (a) a line tangent to the femoral head and (b) a line that is parallel to the first and runs along through the anterior aspect of the femoral neck.
Source: From Ref. (12). Clohisy JC, Carlisle JC, Beaule PE, et al. A systematic approach to the plain radiographic evaluation of the young adult hip. J Bone Joint Surg Am. 2008;90(Supp 4):47–66.
Muscular and Movement Pattern Differences
Just as there are bony gender differences of the hip, neuromuscular differences exist as well. Even among highly trained athletes, females tend to have relatively weaker hip abductors (20). This leads to a predictable movement pattern during single-leg squats, drop landings, and side-step cutting activities: females tend to have greater hip adduction and internal rotation, greater knee abduction, and less trunk and hip flexion (21,22) (see Figure 7.9). They also generate smaller hip extensor moments, and during side-step cutting activities females usually have pelvic rotation and trunk-lean toward the weight-bearing limb, whereas males have pelvic rotation and trunk-lean toward the non-weight-bearing limb (22,23). This combination of movements in females requires more force generation by the knee extensors and puts more stress on the knee joint (21).

FIGURE 7.5: Femoral offset. Femoral offset describes the horizontal separation between the femur and the acetabular socket. It is the perpendicular distance from the rotational center of the femoral head to a line drawn along the longitudinal axis of the femoral shaft.
Source: From Ref. (10). Atkinson HD, Johal KS, Willis-Owen C, et al. Differences in hip morphology between the sexes in patients undergoing hip resurfacing. J Orthop Surg Res. 2010;5:76. With permission from BioMed Central.
One possible contributor to females’ relative hip abductor weakness is the gender difference in bony anatomy. Because females have a bigger pelvic width-to-femoral length ratio, females must generate more torque across the hip in order to maintain a level pelvis (3). But, by increasing trunk flexion during squat-type activities, females can generate a pattern of energy absorption that is more similar to the typical male pattern. This is important because adapting a movement pattern to increase trunk flexion during squat activities may decrease females’ risk of lower extremity injury (24).
In addition to gender differences in hip muscle strength, there are also differences in muscle stretch and possibly differences in laxity of other surrounding soft tissue structures. Females have lower passive hamstring stiffness (25,26) and higher tolerance to stretch (27). They also have increased prevalence of symptomatic extra-articular impingement between the femur and contact points on the pelvis such as the ischial tuberosity and anterior inferior iliac spine. Eighty-five percent of diagnoses of extra-articular impingement are made in females. Some hypothesize that increased peri-articular soft tissue laxity may contribute to females’ increased risk of encountering bony impingement during activities in end ROM (28).

FIGURE 7.6: Acetabular version. Acetabular version is calculated from an axial image. It is the angle between (a) a line perpendicular to the plane of the ischial tuberosities and (b) a line connecting the anterior and posterior margins of the bony acetabulum.
Source: From Ref. (10). Atkinson HD, Johal KS, Willis-Owen C, et al. Differences in hip morphology between the sexes in patients undergoing hip resurfacing. J Orthop Surg Res. 2010;5:76. With permission from BioMed Central.
Females are also more likely to have generalized joint laxity (29). Though not quantified at this time, it is possible that females experience hip dysfunction related to joint laxity more commonly than males. Further studies are needed to better assess and determine these potential differences (Table 7.2).

FIGURE 7.7: Lateral center-edge angle (CEA). The lateral CEA is calculated from an AP radiograph. It is the angle between (a) a vertical line drawn through the center of the femoral head and (b) a line connecting the center of the femoral head and the outer edge of the acetabular roof.
Source: From Ref. (12). Clohisy JC, Carlisle JC, Beaule PE, et al. A systematic approach to the plain radiographic evaluation of the young adult hip. J Bone Joint Surg Am. 2008;90(Supp 4):47–66.
INTRA-ARTICULAR DISEASE—PREARTHRITIC CONDITIONS
While the etiology of degenerative hip OA in a given patient remains idiopathic, studies are now showing an association between early onset of hip OA and preexisting hip deformity. Some of these “prearthritic” symptomatic hip conditions occur at a disproportionately high rate in young athletes, so understanding these disorders is essential in order to appropriately manage these athletes and minimize the effect on the duration and intensity of their playing careers. This section discusses prearthritic hip conditions that have research-supported sex differences.
Legg-Calvé-Perthes Disease
Legg-Calvé-Perthes disease (LCPD) is osteonecrosis of the femoral head epiphysis in children and young adolescents. The peak age at diagnosis is 5 to 8 years old. The etiology is still unclear, but the leading hypothesis is repetitive microvascular trauma to the femoral head, possibly due to increased intra-articular pressure (30). LCPD is four to nine times more common in males than females, and males are more likely to have bilateral LCPD (31,32). However, females tend to have a worse prognosis (33,34), possibly because the female proximal femoral physis closes at a younger age, which leaves a shorter potential period for remodeling of the femoral head (31). In contrast, the male sex is associated with more severe intra-articular hip disease in people with Perthes-like hip deformities. Perthes-like hip deformities include other causes of vascular insult to the proximal femur during skeletal development such as infection, trauma, and complications of treatment for hip dysplasia (35).

FIGURE 7.8: Acetabular inclination described by Tönnis angle. Acetabular inclination described by the Tönnis angle is calculated from an AP radiograph. To calculate this angle, first establish the transverse pelvic axis by drawing a line connecting the right- and left-sided acetabular teardrops (Line 1). The Tönnis angle is the angle between (a) a line that is parallel to the transverse pelvic axis and that crosses through the inferior aspect of the acetabular sourcil (i.e., the sclerotic weight-bearing aspect of the socket), and (b) a line connecting the medial and lateral aspects of the acetabular sourcil. A normal angle is 0° to 10° (12).
Source: From Ref. (12). Clohisy JC, Carlisle JC, Beaule PE, et al. A systematic approach to the plain radiographic evaluation of the young adult hip. J Bone Joint Surg Am. 2008;90(Supp 4):47–66.
TABLE 7.1: Sex Differences of Bony Hip Anatomy
Proximal Femur | |
Alpha angle (“bulkiness” of femoral head-neck junction): Greater in males Femoral version (“twisting” of the femur): Unclear Femoral head-neck offset (taper of the femoral neck): No difference Femoral offset (horizontal separation between femur and acetabulum): Greater in males Femoral neck width: Greater in males | |
Acetabulum | |
Acetabular anteversion angle (anterior angle of socket opening): Greater in females Acetabular retroversion (posterior angle of socket opening): More frequent in males Acetabular lateral center-edge angle (amount of femoral head coverage): Unclear Acetabular Tönnis angle (vertical tilt of socket opening): No known difference Articular surface area: Greater in males Acetabular development: Earlier in females | |
Range of Motion | |
Greater in females: Hip flexion Hip internal rotation at 90° flexion Greater in males: Hip extension Hip external rotation at 90° flexion | |
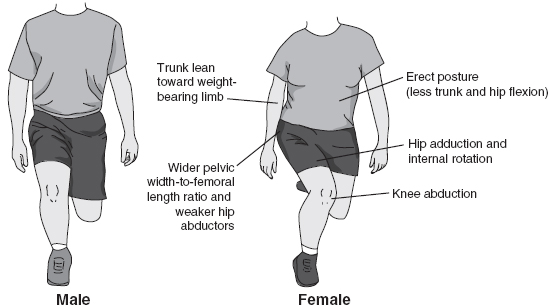
FIGURE 7.9: Movement pattern implications of common sex differences of pelvic anatomy and hip strength.
TABLE 7.2: Sex Differences of Strength and Movement Patterns Around the Hip
Compared to males, females have: |
Weaker hip abduction Lower hamstring stiffness Higher tolerance to hamstring stretch |
During squat exercises, compared to males, females have: |
Greater hip adduction and internal rotation Greater knee abduction Less trunk flexion Smaller hip extensor moments Increased stress on knee joint |
During side-step cutting: |
Females have: Pelvic rotation and trunk-lean toward weight-bearing limb Males have: Pelvic rotation and trunk-lean toward non-weight-bearing limb |
Since the pathophysiology of LCPD is unknown, research has focused on studying potential risk factors and associations between LCPD and other conditions. It is hypothesized that children who are more hyperactive have an increased frequency of microtrauma and stress to the vascular supply to the hip joint. Supporting this theory, people with LCPD have an increased prevalence of attention deficit hyperactivity disorder (ADHD) and a higher risk than the general population for hospitalization due to other lower extremity injuries. Both of these associations are stronger in females (30,36), even though the actual prevalence of LCPD, ADHD, and injuries requiring hospitalizations is higher in young males.
Slipped Capital Femoral Epiphysis
Similar to LCPD, SCFE is a condition affecting prepubertal children. It is the displacement between the femoral head and femoral neck at the growth plate, in which the femoral head remains in the acetabulum but the rest of the femur shifts anteriorly and rotates externally. It is well established to be most common in obese children around the time of puberty (37).
SCFE is about 1.5 times more common in males than females in the United States (38). This male predominance is present in Mexico, Japan, and Korea as well. The trend was not reproduced in the Netherlands, but this is likely because over the time period of the study, the incidence of SCFE in females rose (37,39–41). Unfortunately, SCFE is occurring more frequently and at younger ages worldwide, and these trends correlate with the rising rate of childhood obesity in each of the countries studied.
Femoroacetabular Impingement
Femoroacetabular impingement (FAI) is a term that describes a hip structural aberrancy measured by radiographic imaging. There is some confusion in nomenclature because the term is also often used to describe a bony condition associated with symptoms, even though 30% of an asymptomatic population has been found to have FAI on radiographs (4). In people with hip pain and FAI on their radiographs, their symptoms are thought to be related to contact between the proximal femur and the acetabular rim during hip movement and loading. Over time, this can lead to acetabular labral tears, femoral and acetabular chondrosis, and OA. There are three structural subtypes of FAI: cam, pincer, and mixed (see Figure 7.10).
Cam-Type FAI
Cam-type FAI describes the presence of extra bone along the femoral head-neck contour. Commonly called a “pistol grip” deformity, cam-type FAI is most commonly characterized radiographically by a large alpha angle. As mentioned earlier in the chapter, there is not yet a clear alpha angle cutoff value to definitively diagnose cam-type FAI by imaging, but a consensus of experts considers an alpha angle of greater than 60° to define FAI (4). Cam lesions are most common along the anterosuperior plane of the femur, and higher alpha angles directly correlate to increased risk of symptomatic FAI and subsequent cartilage damage (6).
Symptomatic cam-type FAI is most common in young, active males (42–44). It is not clear why there is a gender disparity. One theory is that cam deformities develop from participating in high-impact sports during adolescence because this kind of activity exposes the femur to intense loading during skeletal development (45–47). In the past, boys have been more involved in these high-impact sports, which would be consistent with the higher prevalence of cam-type FAI in males. However, this participation gap is narrowing, so if the hypothesis is correct, the gender difference in cam-type FAI should narrow, too. Another theory to explain the gender disparity is that cam deformities are subclinical slipped capital femoral epiphyses, which are also more common in boys. Since SCFE is more common in sedentary, overweight children as opposed to active youth involved in high-impact sports, this theory somewhat contradicts the first (6).

FIGURE 7.10: Types of femoroacetabular impingement. (A) Normal hip without FAI. (B) Cam-type FAI describes extra bone along the femoral head-neck contour. (C) Pincer-type FAI describes overcoverage of the femoral head by the acetabulum. (D) Mixed-type FAI describes the coexistence of both cam and pincer abnormalities in the same hip.
Source: From Ref. (128). Lavigne M, Parvizi J, Beck M, et al. Anterior Femoroacetabular Impingement: Part I. Techniques of Joint Preserving Surgery. Clin Orthop Relat Res. 2004;418:61–66.
Pincer-Type FAI
Pincer-type FAI describes overcoverage of the femoral head by the acetabulum. It is commonly defined radiographically by a lateral CEA of at least 40° or a Tönnis angle less than 0° (48). Pincer-type FAI is more common in middle-aged females. Again, the etiology of this gender discrepancy is unknown. In fact pincer-type FAI is commonly associated with acetabular retroversion, and as mentioned previously, acetabular retroversion is more common in males even though they have a lower prevalence of pincer-type FAI (13).
Mixed-Type FAI
Although it is thought that cam and pincer deformities have different etiologies, they commonly exist simultaneously in the same hip. This is called mixed-type FAI and is more common in males (49,50). Reporting of prevalence and outcomes of people with mixed deformity is evolving. In a 2009 study by Allen et al., 42% of hips with cam deformities also had a pincer deformity (51). In a study by Byrd and Jones in 2011, there were 159 cam, 10 pincer, and 31 combined lesions (52).
Sex Differences in Symptomatic FAI Clinical Presentation
Just as asymptomatic females may have smaller “normal” alpha angles than males, females with symptomatic FAI tend to present with pain and labral tears associated with smaller alpha angles as compared to males with symptomatic FAI (49,53). Hetsroni et al. theorize that females’ increased sensitivity to develop symptoms associated with smaller alpha angles may be due either to weaker hip stabilizing muscles, leading to increased force through the hip joint, or to increased soft tissue laxity and subsequent greater ROM, allowing frequent contact of the proximal femur and the acetabulum (53). Another theory is based on the observation that pincer-type FAI causes more direct damage to the labrum compared to cam-type FAI, which tends to cause more separation between the labrum and articular cartilage. Because the labrum is richly innervated by nociceptive fibers, pain is likely to be more severe after direct damage to the labrum. Pincer-type FAI is more common in women and may be a more painful form of FAI. (54).
Despite females’ increased predilection for pain and labral pathology associated with small cam lesions, males tend to have more severe structural abnormalities at the time of presentation. This includes more severe cam lesions, a higher frequency of labral tears, and more advanced acetabular hyaline cartilage lesions (49,55,56). Males are also more likely to develop bilateral symptomatic FAI (57). Advanced intra-articular cartilage injury and degeneration is a poor prognostic factor for satisfactory joint preservation surgery outcomes, so as a result this gender difference in injury and degenerative severity at presentation is important to consider when counseling patients regarding treatment options.
Interestingly, though males tend to have more severe structural abnormalities, FAI has a larger impact on quality of life in females (58). In patients who decide to proceed with hip preservation surgery, postoperative quality of life measures are still lower in females than males (59). This draws further attention to the need for prospective studies related to gender-specific differences and needs in order to improve outcomes.
Developmental Dysplasia of the Hip
Like FAI, developmental dysplasia of the hip (DDH) is a hip deformity associated with intra-articular pain and also is a known risk factor for the development of OA. However, in contrast to the excessive contact between the femur and acetabulum as in FAI, DDH is characterized by inadequate femoral head coverage by the acetabulum. DDH is commonly defined radiographically as a lateral CEA less than 25° or, in severe cases, less than 20°.
DDH is more common in females than males, regardless of patients’ age at presentation (60). Diagnosis of DDH is often made in infancy during routine screening exams. In this population, females have a 2.5- to 4-fold increased risk of DDH (61–63). Sometimes, though, DDH is not diagnosed until a person develops hip pain in adolescence or early adulthood. In this group of older patients, the female predominance is present but less pronounced (60). While risk factors for DDH have been identified, the exact etiology remains unclear. In light of this difference in gender demographics based on patients’ age at presentation, it is possible that DDH diagnosed in young adults is a distinct condition that develops after infancy, rather than a milder version of the condition diagnosed with newborn screening exams (60,64).
Aside from research proving the female predominance of DDH, there have been few gender-focused studies on this condition. From the scattered research that has been done, it seems there is no gender difference in clinical response to the Pavlik harness in infants (65) or to hip preservation surgery—namely, eccentric rotational acetabular osteotomy—in young adults (66). There is, however, a stronger association between DDH and subsequent degenerative joint-space narrowing in females than males (67). Females with DDH also have a higher incidence than the general population of spina bifida occulta, but this association is not seen in males (68). The reason for this gender difference is unknown, but it could help identify at-risk newborns who would benefit from hip screening programs through adolescence.
Acetabular Labral Tear
The acetabular labrum is a ring of cartilage around the outer rim of the bony acetabulum. It serves to deepen the hip socket and provide increased area of contact between the femoral head and hip socket. Even in hips with normal bony structure the labrum can become damaged from repetitive mechanical stress and trauma, but abnormal hip structure such as FAI and DDH deformities further expose the labrum to increased load and risk for tear (69). Labral tears are clinically important because they can be painful, limit patients’ desired activity, and predispose to degenerative OA.
The sex differences in patients with acetabular labral tears mirror those seen in people with normal hips and with FAI: Males have larger alpha angles and generally less acetabular anteversion (4). There is no gender difference in CEA (53). Most labral tears occur in the setting of hip deformity. When presenting for surgery for labral tears, males tend to have larger tears (70) but females require a longer recovery period (71). Again, it is important to be aware of these differences in order to optimally manage and counsel patients. Specifically, females with hip pain and only mild cam-type FAI deformities on imaging still warrant suspicion and evaluation for labral tears, and recovery time estimates after FAI surgery can be tailored by gender.
There are also special patient populations who are at increased risk of acetabular labral tears and have uneven gender representation. First, labral tears can occur during pregnancy and labor (72). Physiological increased ligamentous laxity and altered cartilage matrix may play a role in peripartum labral tears (73), and laboring positions involving extreme hip flexion and internal rotation also increase the risk for acute tears. Women who have epidural anesthesia will not experience the pain right away and may only notice hip dysfunction as they become more active again. Second, dancers have a high prevalence of labral tears. In this population, especially at the professional level, labral tears appear to more often be the result of repetitive joint stress at extreme ranges of motion in structurally normal hips, rather than the result of bony deformity such as FAI or DDH. Also, labral tears in this population occur more frequently in the superior and posterosuperior region, rather than in the anterior and anterosuperior region as in the general population (74) (Table 7.3).
INTRA-ARTICULAR DISEASE—OSTEOARTHRITIS
Epidemiology
The entities of LCPD, SCFE, FAI, DDH, and acetabular labral tears described here are considered prearthritic hip diseases because they all increase a person’s risk for developing degenerative hip OA. Not surprisingly, since there are sex differences in the conditions that predispose to hip OA, there are also sex-specific differences in the prevalence and manifestations of hip OA.
TABLE 7.3: Sex Differences in Pre-Arthritic Hip Disorders
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


