Chapter 20. Granulomatous disorders and tumours
Granulomatous conditions
There are three disorders of the reticuloendothelial system that affect bone; all are rare, but they are important because they can be mistaken for tumours:
1. Eosinophilic granuloma.
2. Hand–Schüller–Christian disease.
3. Gaucher’s disease.
Eosinophilic granuloma
The lesions of eosinophilic granuloma are ‘punched-out’ holes in the skull and elsewhere. Radiologically, the lesions resemble metastases or bone cysts (Fig. 20.1). The ‘holes’ contain a soft brown tissue.
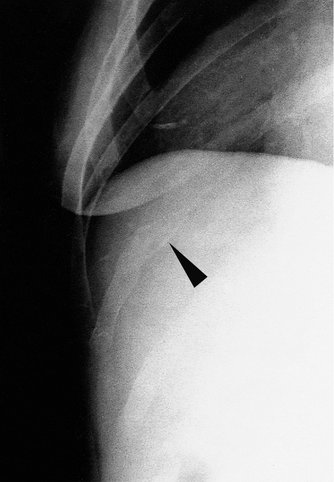 |
| Fig. 20.1 Eosinophilic granuloma of the rib. |
The condition is not fatal and may regress spontaneously.
Hand–Schüller–Christian disease
This condition is similar to eosinophilic granuloma except that the lesions are paler and the brain is often involved, particularly around the pituitary. The condition is slowly progressive and may be fatal.
Gaucher’s disease
Gaucher’s disease is a systemic disorder in which an abnormal fatty substance (kerasin) is deposited in the liver and other tissues. Bone involved in Gaucher’s disease contains irregular cysts and cavities visible radiologically. Affected bones, particularly the femoral head and condyles, may collapse and make joint replacement necessary.
Tumours
Radiological appearance of bone tumours
When looking at bone tumours on a radiograph, ask the following questions:
Classification of bone tumours
The classification of bone tumours should reflect the cell of origin. They can be further subclassified into benign and malignant tumours (Table 20.1).
| Benign | Malignant | |
|---|---|---|
| Fibrogenic | Simple cyst | Malignant fibrous |
| Aneurysmal bone cyst | Hystiocytoma | |
| Fibrous dysplasia | ||
| Fibrous cortical defect | Fibrosarcoma | |
| Chondrogenic | Enchondroma | Chondrosarcoma |
| Periosteal chondroma | ||
| Osteochondroma | ||
| Chondromyxoid fibroma | ||
| Chondroblastoma | ||
| Osteogenic | Osteoid osteoma | Osteosarcoma |
| Osteoblastoma | ||
| Ossifying fibroma | ||
| Unknown origin | Giant cell | Ewing’s |
| Synovial sarcoma | ||
| Bone marrow | Myeloma | |
| Lymphoma |
Simple bone islands (Fig. 20.2) are of no particular significance, although they are often striking on X-ray.
 |
| Fig. 20.2 Cortical bone islands. |
Benign bone tumours
Fibrogenic
Fibrous cortical defect (Fig. 20.3). This most common abnormality has a characteristic oval X-ray appearance with a sharp margin and often multilocular. No specific treatment is required.
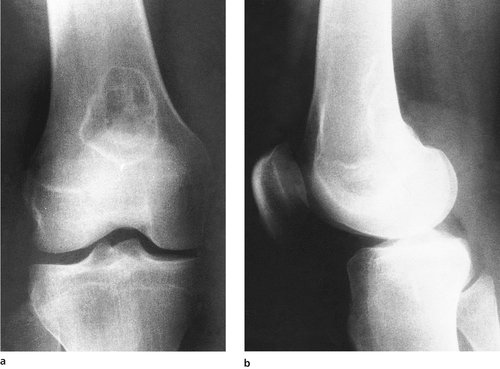 |
| Fig. 20.3 (a), (b) Fibrous cortical defect at the lower end of femur. |
Fibrous dysplasia. This can present in mono- or polyostotic forms and is seen more commonly between the second and third decades. The radiographic appearance is of a ground-glass expansile lesion, often with a bowing of the affected bone. A ‘shepherd’s crook’ deformity is seen in the proximal femur as a result of this bowing and possible multiple fractures. The polyostotic form can be associated with hypothyroidism, vitamin D-resistant rickets and the Cushing syndrome. Albright’s syndrome includes the polyostotic dysplasia with café-au-lait spots and precocious puberty. The lesions are reasonably characteristic on X-ray but occasionally a biopsy is required. When painful, these are adequately treated with curettage and bone grafting. Occasionally there can be an associated fracture, although this is rare.
Simple bone cyst (Fig. 20.4). These cysts may occur during growth and are commonly located adjacent to the epiphyseal plate. They are usually asymptomatic until pathological fracture occurs. The radiographic appearances show a well defined radiolucent lesion, often with this pathological fracture.
 |
| Fig. 20.4 (a) A pathological fracture through a simple bone cyst of the humerus; (b) the fracture has united and the bone cyst is less obvious. |
Bone scans confirm a decreased uptake in the area and treatment is unnecessary unless there is a risk of fracture. These cysts can heal spontaneously after a fracture, but when in doubt aspiration and an injection of methylprednisolone acetate has an 80–90% success rate. Curettage and bone grafting is occasionally necessary.
Aneurysmal bone cyst (Fig. 20.5




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
