Chapter 18 Gender Differences in Muscular Protection of the Knee
PROPRIOCEPTION
Proprioception refers to an individual’s awareness of joint and body movement and their position in space. Motor control feedback via the gamma motor system can modify muscle stiffness or transjoint resistance of muscles to control joint movement and positioning during planned and unexpected events. Therefore, skeletal muscle plays an important role in knee joint proprioception. An individual’s ability to detect knee joint position and motion is a major component required for reflex response, allowing joint stabilization and protection to develop. When errors in these systems occur, or when these systems function at suboptimal levels, increased ligament strain, articular cartilage shear, and/or bone impact may result. High risk positioning of the lower extremity may also occur.13,20
Critical Points PROPRIOCEPTION
Several authors have reported gender differences in proprioception.21,39,40,53 Rozzi and coworkers40 investigated joint proprioception in 34 (17 male, 17 female) collegiate soccer and basketball athletes by measuring the threshold to detection of passive motion using a device that moved the knee joint at a constant 0.5°/sec velocity through flexion and extension. A rotational transducer provided angular displacement values. Compared with male athletes, females took significantly longer to detect the threshold of knee joint motion in extension (2.11° ± 0.63° and 2.95° ± 1.47°, respectively; P = .039). However, no significant gender difference was observed during flexion. The clinical significance of a mean difference of 0.84° of angular motion between genders is unknown.
Hewett and associates21 assessed proprioception using single-leg postural balance at the knee on a dynamic platform in ACL-deficient subjects. Uninjured females demonstrated greater knee joint stability than males, which the authors attributed to a lower center of gravity. In contrast, males had significantly greater single-leg stability after an ACL rupture, and females took longer to regain adequate levels of single-leg balance postoperatively.21 A clear gender difference cannot be extracted from these results.
Although injury research often focuses on the lower limbs, the core of the torso may be the key to understanding body positioning. Therefore, the core muscle of the torso should not be overlooked in the investigation of proprioception. Zazulak and colleagues53 evaluated core proprioception and knee joint control. Two-hundred seventy-seven collegiate athletes (137 male, 140 female) underwent core proprioceptive measurements by passive trunk rotation in the seated position through 20° in the transverse plane. With auditory and visual stimuli diminished, the athletes were instructed to reproduce the initial position after displacement. The difference between the perceived and the actual angle was calculated as the active proprioceptive repositioning error. After testing, the athletes were followed for 3 years, during which 25 (14 male, 11 female) sustained knee injuries. Analysis of the active proprioceptive repositioning error revealed that females who sustained knee ligament or meniscal injuries demonstrated significantly greater error in active repositioning than uninjured females. Male athletes did not demonstrate this problem. In addition, uninjured female athletes had significantly better core proprioception than uninjured male athletes, which supports previous studies.20,40 Zazulak and coworkers52 also reported that after an unexpected perturbation, the maximal trunk displacement in females who suffered knee ligament injuries was significantly greater than that of females who did not experience injury. No significant difference in maximal trunk displacement between injured and uninjured males was found. Therefore, the core stability of female athletes may be a greater factor in lower extremity injury susceptibility than that in males.52 In fact, lateral trunk displacement was the lone significant predictor of ligament injury in female athletes (P = .001) in this investigation, with 100% sensitivity and 72% specificity rates reported. This was not true for male athletes, because their sole predictor of injury was a history of low back pain.52
Other factors that may influence proprioceptive function include joint laxity and muscle fatigue, both of which also affect muscle function. Rozzi and associates39 reported that female athletes had greater knee laxity that resulted in a decreased sensitivity to knee position change. Many clinicians have suspected that joint laxity is a risk factor for knee injury, but the evidence is not overwhelming. The best evidence may be that provided by Uhorchak and colleagues43 in their risk factor analysis for ACL injury in military cadets.
Regarding muscle fatigue, Rozzi and associates39 showed in male and female collegiate basketball and soccer athletes that induced fatigue altered proprioception, especially in knee extension. Wojtys and coworkers51 evaluated the effects of muscle fatigue on anterior tibial translation, muscle reaction time, and recruitment order in 10 athletes (6 male, 4 female) whose physical activity included jumping, pivoting, and twisting. Each athlete completed baseline measurements and then underwent a vigorous isokinetic workout until quadriceps and hamstrings torques decreased by 50% or greater. Eight of the 10 fatigued athletes demonstrated greater anterior tibial translation during dynamic testing (average percentage increase, 32.5%), indicating that fatigue did increase joint laxity. Fatigued athletes did not alter their muscle recruitment order in response to an anterior tibial translation. However, after fatigue, muscle reaction time slowed significantly in the three response phases (spinal reflex, intermediate, and voluntary). Although the investigation found a change in muscle reaction time and laxity of the knee, no gender difference was reported for these factors, nor was a correlation established between fatigue and a decrease in proprioception.
Earlier studies have evaluated the effect of ACL-deficiency on proprioception, although gender was not specifically examined.6,11,48 More recent studies have focused on gender differences. In general, these studies show that injured female athletes have poorer lower extremity proprioception than their male athlete counterparts.21,40,52 However, uninjured female athletes tend to have higher levels of stability than healthy male athletes.
Considering the consequences of serious knee injury, proprioceptive prescreening of female athletes, especially in high-risk sports, prior to athletic participation may help focus training and conditioning programs.20,52,53
MUSCLE RESPONSE
Time to Peak Torque
Neuromuscular activation patterns influence dynamic knee joint stability potential, which may contribute to knee injury susceptibility.10,19,23,25 Gender-related differences in these activation patterns have been reported by numerous investigators.8,10,27,33,40,41,44,47
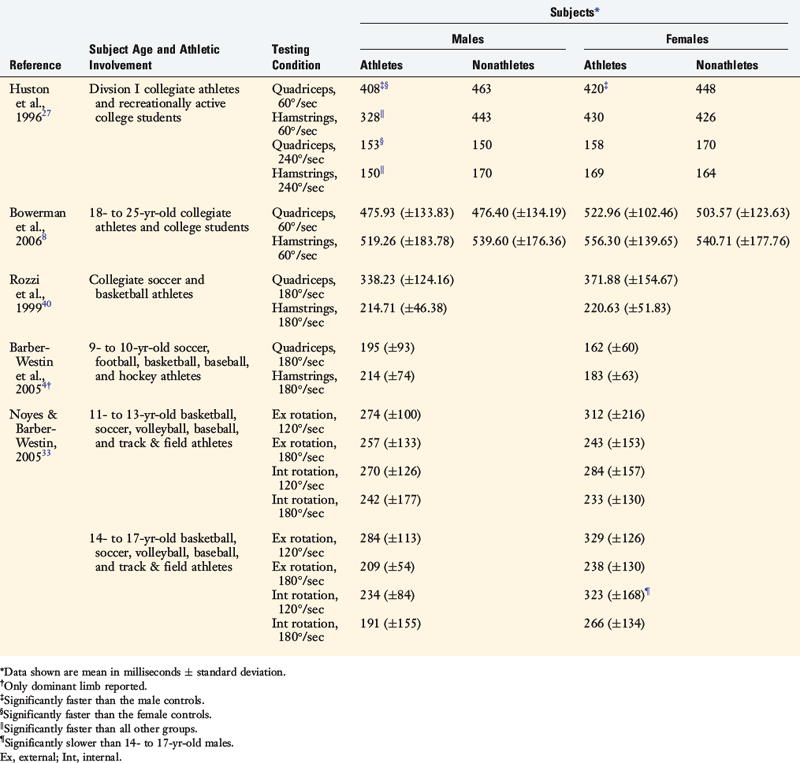
Using isokinetic peak torque strength testing of 100 Division I athletes (60 male, 40 female), Huston and Wojtys27 detected significant gender differences. Female athletes and controls generated similar time to peak knee flexion torques, which were slower than male athletes. Male athletes were able to generate peak knee extension and flexion torques faster than male or female controls (Table 18-1). The slowed response of the hamstring in females was most striking.
Critical Points MUSCLE RESPONSE
Considering the young age at which many ACL injuries occur, muscle function maturation should be considered in the evaluation of injury susceptibility. Noyes and Barber-Westin33 examined the gender- and age-related differences in time to peak torque for internal and external tibial rotation with isokinetic strength testing. They separated 94 athletes into two age groups: 11 to 13 years of age (20 male, 20 female) and 14 to 17 years of age (27 male, 27 female). Older male athletes were faster (28%) in internal rotation peak torque of the hamstrings than age-matched female athletes (see Table 18-1). In contrast, multiple investigators have reported no gender differences in isokinetic peak torques for quadriceps and/or hamstrings in collegiate athletes,8,40 nonathlete controls,8 and athletes 13 years of age or younger4,33 (see Table 18-1).
Muscle Reaction Time
In an attempt to identify more relevant functional gender differences, several investigators have assessed peak muscle torque during weight-bearing perturbations and athletic tasks. Shultz and associates41 examined muscle response times in 64 collegiate lacrosse and soccer athletes (32 male, 32 female) after applying an unexpected rotational perturbation force to the lower extremity. Female athletes’ muscle response times for the quadriceps muscles were faster than male athletes with comparable recruitment patterns (Table 18-2). The Division I collegiate athletes displayed faster muscle response times than the recreational athletes.
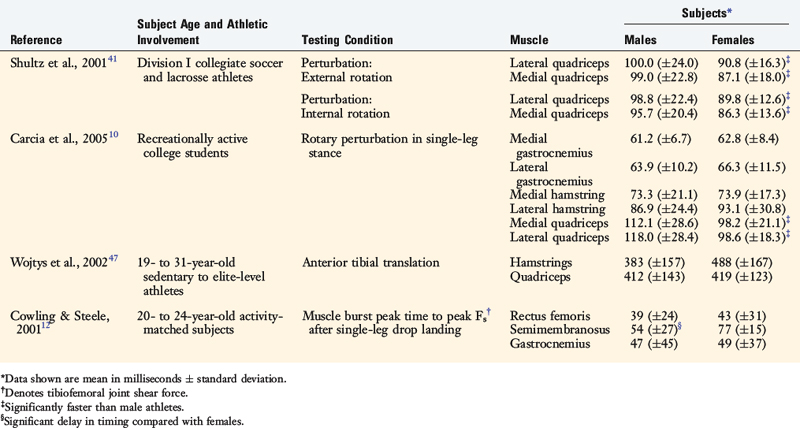
Carcia and colleagues10 measured the response times of the quadriceps, hamstrings, and gastrocnemius muscles after a weight-bearing rotary perturbation in 20 recreationally active adults (10 male, 10 female). Males and females responded with similar muscle recruitment order patterns at various angles of flexion (10°, 20°, 30°), and females generated faster quadriceps muscle response times than males at all angles (see Table 18-2).
Using a posterior force to the calf muscle to simulate anterior tibial translation, Huston and Wojtys27 reported that female athletes activated their quadriceps first and faster than their male counterparts, raising concerns about what role the quadriceps could directly play in ACL injuries. In contrast, Cowling and Steele12 reported a delay in the semimembranosus (hamstring) muscle of male athletes during abrupt single-leg landing compared with athletic level–matched female athletes.
In summary, preferential quadriceps activation and a slowed hamstring response may lead to a neuromuscular imbalance producing ineffective knee stabilization.10,27,41,49 Powerful or unopposed quadriceps contractions, especially close to knee extension, have the potential to cause ACL injury.46 Further research is necessary to better understand these relationships, especially in terms of muscle activity mode injury rates.
Strength
The timely ability to generate high levels of muscle force across the knee joint may decrease functional joint laxity and result in less stress and strain on the passive structures that constrain knee motion.7,8,15,16,27,47,49 A poor muscle strength–to–body weight ratio may be a risk factor for lower extremity injury.30,43
Besides the peak torque–to–body weight ratio, the balance of forces expressed as the hamstring-to-quadriceps (H:Q) ratio is an additional performance measurement that may provide insight into the gender differences in injury susceptibility. Evidence suggests that the hamstring muscles have the potential to unload the ACL,46 whereas the quadriceps appear to function as the ACL antagonist.46 The suspected relationship between the H:Q peak torque ratio and ACL injury susceptibility has been investigated by several authors.2,8,9,22,38 This factor may be critical in ACL protection.2,4,5,8,9,22,38,49
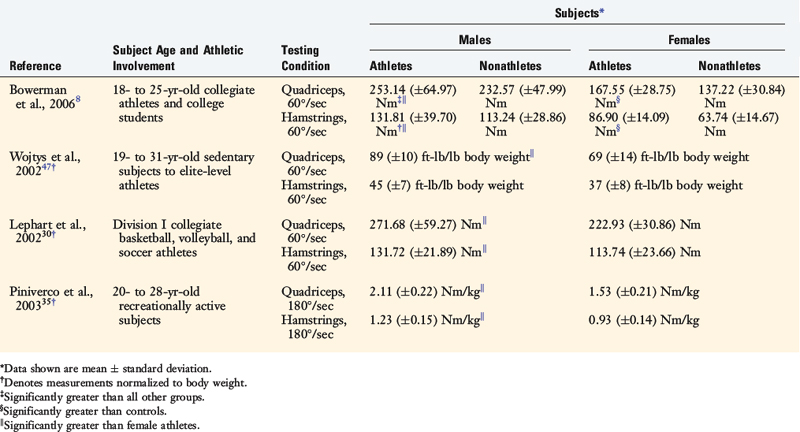
Bowerman and coworkers8 tested the peak isokinetic muscle torque (60°/sec) of 54 healthy collegiate athletes and 53 age-matched nonathletes. Males were stronger than females for both quadriceps and hamstring muscles (Table 18-3). Unfortunately, measurements were not normalized to body weight in this study. Not surprisingly, athletes generated higher quadriceps and hamstring peak torques. Similar findings were reported by Wojtys and associates47 in 23 healthy volunteers (10 male, 13 female) whose activity level ranged from sedentary to elite-level athletes. Lephart and colleagues30 also reported similar results, as did Bowerman and coworkers8 in 15 Division I collegiate athletes and 15 age-matched male controls under the same testing conditions after normalizing for body weight (see Table 18-3). Male recreational athletes generated greater quadriceps and hamstring peak isokinetic torques (180°/sec) than their female counterparts with body weight normalization.35 In addition, Hewett and coworkers22 and Anderson and associates2 reported that female high school athletes had lower H:Q ratios than male athletes. Conversely, Bowerman and coworkers8 and Rosene and colleagues38 found no gender difference in H:Q ratios among collegiate soccer, volleyball, softball, basketball, football, tennis, and track athletes. However, their strength levels were not corrected for body weight (Table 18-4).
< div class='tao-gold-member'>
Related posts:
 Allografts: Graft Sterilization and Tissue Banking Safety Issues
Differences in Neuromuscular Characteristics between Male and Female Athletes
The International Knee Documentations Committee Rating System
Knee Ligament Function and Failure
Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes
Allografts: Graft Sterilization and Tissue Banking Safety Issues
Differences in Neuromuscular Characteristics between Male and Female Athletes
The International Knee Documentations Committee Rating System
Knee Ligament Function and Failure
Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


