THE SELF-REGULATORY EXECUTIVE FUNCTION MODEL
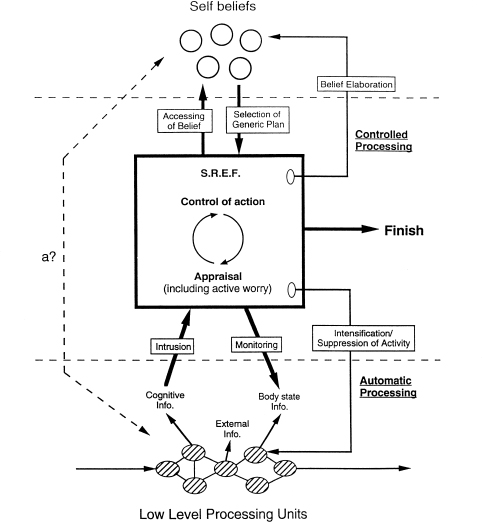
Wells and Matthews (1994) developed the self-regulatory executive function (S-REF) model to represent the interactions between appraisals, attentional control, and beliefs in the maintenance of emotional disorder. Figure 10.0 presents an outline of the model.
Three levels of processing are distinguished in the model: a level of automatic processing of external and internal stimuli, a level of controlled processing involved in the regulation of behaviour and thought, and a store of beliefs that guide the content and activities of the controlled processing system. Automatic processing is rapid and occurs outside of conscious awareness, although the output of automatic processing may intrude into consciousness. Highly practised activities acquire partial automaticity; for instance, the actions necessary for driving a car become more reflexive with practise, require less conscious involvement, and demand less attention. Fully automatised processing is not amenable to consciousness, and requires no attention, but it is unlikely that the processing that occurs in emotional disorder is ever fully automatised since it involves complex processing operations that are influenced by changing patterns of internal and external information. Controlled processing is synonymous with attentionally demanding appraisals that are amenable to consciousness, although some patients report diminished awareness of such on-line appraisals initially. The execution of appraisals relies on the accessing of beliefs that shape the content and nature of appraisals and behavioural responses. For example, a social phobic may appraise the occurrence of sweating as an indication that he/she looks ‘abnormal’, while a non-phobic may appraise the same event as an indication that he/she looks hot. In each case the appraisals are based on beliefs concerning the meaning and significance of the bodily event. On the basis of these appraisals behavioural responses are tailored to deal with the situation, and are executed within the controlled processing system. Some of the behavioural and cognitive coping strategies executed are problematic because they prevent exposure to experiences that can disconfirm dysfunctional beliefs, or they affect the processing system in ways that maintain unhelpful modes of processing. For instance, the use of rumination or active worry as a coping strategy may drain the attention needed for processing disconfirmatory information, and can maintain preoccupation with, or increase attentional bias for threat. Verbal rumination may distract attention away from processing emotional information (intrusive images) such that emotional processing is retarded and symptoms of failed emotional processing, such as intrusive thoughts about stress, proliferate (e.g. Borkovec & Inz, 1990; Wells & Papageorgiou, 1995).
Figure 10.0 The S-REF model (Wells & Matthews, 1994)
A benefit of articulating the dynamic interplay between levels of cognition in models like the S-REF is that it offers a preliminary working framework for understanding how cognitive processes and structures interact in the maintenance of disorder. Armed with this type of knowledge, predictions can be made concerning not only what should be done in cognitive therapy but also how cognitive change may be best achieved through manipulating interacting components of the system. In the S-REF model a particular mode of processing termed the S-REF is thought to be activated in emotional disorder. This mode consists of the activation of self-relevant beliefs, the appraisal of internal and external stimuli with respect to these beliefs, and the regulation of appraisal and behaviour intended to overcome any discrepancies between appraised actual and desired states of the self. Thus, S-REF processing serves a self-regulatory function. This function is partly meta-cognitive in its effect in that S-REF processing is capable of regulating and modifying aspects of the processing system, such as priming automatic processing, and the activation, deactivation, or assimilation of new information to existing beliefs. Some beliefs that are activated are primarily meta-cognitive in nature, such as beliefs that it is necessary to worry on an issue in order to cope, or the belief that having particular thoughts will lead to loss of control.
A particular mode of S-REF functioning is purported to underlie emotional disorder. A marker for this processing mode is chronic and intense self-focused attention. The mode comprises perseverative self-referent processing (worry or rumination), activation of dysfunctional self-beliefs and monitoring for threat. The exact content of active worry, beliefs, and the nature of intrusions from automatic processing varies across disorders. For example, threat monitoring in panic disorder includes selective attention to internal bodily events, in obsessional-disorder monitoring consists of selective attention for particular thoughts, while in social phobia there is selfmonitoring of the publicly conspicuous aspects of self. Behavioural responses exert an effect on the processing mode: perseverative S-REF processing is at least partially maintained by choice of coping strategy. We have seen in previous chapters how safety behaviours may exacerbate symptoms, block disconfirmation of belief, and generally maintain or increase discrepancies rather than decrease them over the long term. Some coping responses such as the use of worry or rumination to deal with imagined or objective threat directly contribute to the dysfunctional mode of S-REF activity.
Schema theory considers belief in the form of declarative knowledge such as ‘I’m weak; I’m unattractive; I’m vulnerable; I’m a failure’ stored at the schema level. There is disagreement about how knowledge of this kind is represented in the information-processing system, and some patients have limited insight into the evidence that maintains negative appraisals. Thus, Wells and Matthews (1994) propose that much of the self-belief system exists in ‘procedural’ form, and declarative beliefs such as ‘I’m a failure’ are the result of running particular processing routines. Hence, it is necessary in cognitive therapy to modify the plan or blueprint for the processing routine associated with emotional disorder. Modification of declarative beliefs alone may only be partially effective if the individuals processing routine continues to generate patterns of attention and appraisal that generate dysfunctional knowledge. A panic disorder patient, for example, may be able to concede that he/she rationally knows that he/she will not suffocate in a panic attack, but selective attention, appraisal and safety behaviour responses may be activated during panic that override the reappraisal and make danger tangible once again. The modification of declarative beliefs may represent ‘knowing with the head’ while the introduction of new procedures will support ‘knowing with the heart’. In order to generate and effect changes in procedures it is necessary for the patient to acquire new skills of processing. This will require repeated practise of new processing routines so that new plans can be developed. The modification of attention in treatment provides a central means of interrupting dysfunctional perseverative processing, increasing flexible control over processing, and facilitating the development of alternative processing routines.
TREATMENT IMPLICATIONS OF THE S-REF MODEL
Models of social phobia and generalised anxiety disorder presented in this book are based on concepts derived from the S-REF model. Moreover, treatment implications of managing the patient’s processing configuration as a prerequisite to disconfirmatory processing are clearly represented in the sequential approach adopted in the cognitive therapy of social phobia discussed in Chapter 7. The S-REF model offers a range of implications for cognitive therapy, which are briefly reviewed below.
Managing on-line activity
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


