Chapter 9 Focal Massage Sequences
This chapter is designed to give a number of examples of how soft tissue manipulation (massage) techniques can be used as part of the treatment for specific pathologic situations. Focal massage sequences were defined in Chapter 4 as follows:
DEPLETIVE MASSAGE
An important prerequisite for depletive massage techniques to be effective is the adjunctive use of elevation of the swollen limb. Because gravity tends to promote the collection of edema in the most distal parts of the affected limb, it makes sense that the swollen part should be elevated during treatment and afterward if possible. Elevation means that the swollen tissues must be higher than the patient’s heart. In general, this means that the patient will lie supine on the treatment table and his or her limb will be supported on a bolster or several pillows (see Figure 3-6, B, for an example). It is important that the vessels draining blood and lymph from the swollen area have as straight a path as possible to the heart. Under these conditions, the various strokes are given to the tissues, beginning proximally and working distally to the end of the limb. This concept is depicted in Figure 9-1.
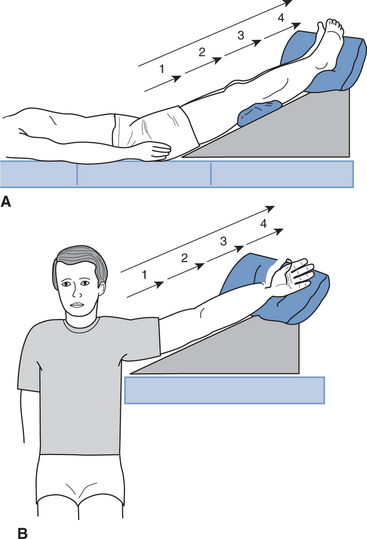
In Figure 9-1, A, the lower limb is divided into four sections, beginning at the thigh and finishing at the foot. The longer the limb, the more sections may be used. Typically, in the lower limb, section 1 would be the upper thigh and section 4 would be the forefoot and toes. Likewise, the upper limb is divided into four sections (Figure 9-1, B). Section 1 would be the upper arm, and section 4 would be the fingers and hand. The limbs are divided in this way to stress the importance of beginning the massage in the proximal sections. The rationale for this approach is that because the tissues are already congested, a pathway needs to be cleared before working on the swollen areas themselves. In this way, the venous and lymphatic channels will be opened to receive the fluids from the swollen areas.
Effleurage to the lower limb is a good example of this idea. Normally the stroke begins distally at the foot and ankle and finishes proximally in the femoral triangle (see Chapter 4). If this technique were applied to a very swollen foot, there would be no space to receive fluids, because the swelling causes collapse of the local capillaries, veins, and lymphatic vessels. The depletive massage concept aims to open up these vessels in the more proximal tissues first, thereby producing open channels that allow the fluids to move. Once the circulation is flowing in a more normal manner, the conventional direction and methods for the various strokes can be used.
At the end of treatment, there is the important issue of how to prevent the return of swelling in the limb when it becomes dependent again. The basic issue is one of pressure in the circulatory system. Essentially, there is a greater pressure (including gravity) forcing fluids into the tissue spaces than there is driving it back into the circulation. Over time, this pressure produces a net accumulation of fluids into the tissues (edema). The pressure tending to drive fluids back into the circulation can be increased with the use of elasticized stockings or socks. Many different types of stockings are available, but they all work in the same basic way. The better ones feature some kind of graduated pressure from distal to proximal in the garment. It is important that such a garment is applied at the end of treatment while the limb is still in elevation. Of course, the patient is instructed to keep the limb elevated as much as possible during the day.
CHRONIC EDEMA
The importance of the lymphatic system in the resolution of chronic edema cannot be overstated. Once the acute inflammatory stage has passed and the capillary walls have closed up, the plasma proteins and other large molecules cannot get back into the capillary network. The only place for them to go is into the lymphatic vessels. In many ways, the lymphatic vessels act as the drainage system for the tissues. Because the lymphatic vessels are thinly walled, without a well-defined valve structure, any massage stroke that involves alternate squeezing and relaxation of pressure will have a powerful effect in promoting flow in this system. However, the normal architecture of the lymphatic system has to be in place for this to work efficiently. Where the lymphatic network has been disrupted, such as may be the case with significant lymph node resection, the swelling may be more widespread and treatment more challeng-ing. This situation is considered at length in Chapter 12, which explores decongestive therapy for the treatment of lymphedema.
Localized, chronic edema can be mobilized using a variety of techniques, including massage. The basic sequence is listed in the tables that follow, and the specific focal massage techniques are italicized. Because the limb is elevated, the therapist may need to stand on a suitable platform, or the therapist may face the patient’s foot and reverse the usual positioning (i.e., by working from knee to hip and from foot to knee). In each case, the massage is always performed from distal to proximal structures (Tables 9-1 and 9-2).
Table 9-1 Focal Massage Sequence for Chronic Edema in the Foot and Ankle Region
| PROCEDURE* | REPETITIONS |
|---|---|
| Depletive stroking to the whole limb | 3 |
| Depletive effleurage to the thigh | 3 |
| Palmar kneading to the thigh | 3 |
| Wringing to the medial thigh | 3 |
| Picking up to the thigh | 2 |
| Depletive effleurage to the thigh | 3 |
| Finger pad kneading around the knee | 3 |
| Palmar kneading to the calf and leg muscles | 4 |
| Thumb pad kneading to the anterior tibial muscles | 4 |
| Picking up to the calf | 4 |
| Depletive effleurage to the thigh, calf, and leg | 3 |
| Finger pad kneading around the ankle region | 4 |
| Thumb pad kneading to the foot | 4 |
| Effleurage to the whole limb | 3 |
Italics indicate specific focal massage techniques.
* Performed with the patient supine and the lower limb elevated.
Table 9-2 Focal Massage Sequence for Chronic Edema in the Forearm and Hand Region
| PROCEDURE* | REPETITIONS |
|---|---|
| Depletive stroking to the whole limb | 3 |
| Depletive effleurage to the upper arm | 3 |
| Palmar kneading to the biceps and triceps | 3 |
| Picking up to the biceps and triceps | 3 |
| Depletive effleurage to the upper arm | 3 |
| Finger pad kneading around the elbow region | 3 |
| Palmar kneading to the forearm muscles | 3 |
| Thumb pad kneading to the forearm muscles | 3 |
| Depletive effleurage to the upper arm and forearm | 3 |
| Thumb pad kneading to the wrist, hand, and fingers | 4 |
| Effleurage to the whole limb | 4 |
Italics indicate specific focal massage techniques.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


