Chapter 11 Connective Tissue Massage
Unlike previous chapters, which have considered the various strokes that make up the method known as Swedish remedial massage, this chapter is the first to focus on a different but parallel system of soft tissue manipulation. Connective tissue massage (CTM)—or in German, bindegewebsmassage—is a total system of specialized soft tissue manipulation techniques originally developed in Europe between the two world wars. It is a good example of a treatment that produces a remote site effect. This concept is well known in many Eastern systems of massage and traditional methods of treatment. Essentially, stimulation given to one part of the body has a profound effect on tissues apparently unrelated to the treatment site. Acupuncture, reflexology, and the more modern concept of trigger point stimulation share this conceptual foundation.
As modern understanding of physiology increases, it is becoming clearer that there is a sound rationale for the use of these concepts, even though they may seem at first glance unlikely. CTM is a significant area of practice, deserving of a book in its own right. As with the other systems of massage described briefly in this text, the intention in this chapter is only to introduce the reader to the basic concepts involved. Many massage textbooks address this topic, but the most comprehensive and authentic materials on the subject in English are still probably the works of Elizabeth Dicke (1978) and Maria Ebner (1985). Other important sources of information in this area can be found in Bischoff and Elminger (1963), Holey (1995b), and Luedecke (1969).
REFLEX ZONES (HEAD’S ZONES)
Since the late 1890s, it has been known that visceral disease can be associated with visible and palpable changes in the skin in well-defined areas of the body. These areas are known as Head’s zones, after Head (1889), who first described them.
As the primitive embryo develops, three layers of tissue begin to differentiate into an outer layer (ectoderm), a middle layer (mesoderm), and an inner layer (endoderm). The ectoderm develops into the skin and nervous system, while the endoderm forms the various internal organs of the body. The middle layer (mesoderm) gives rise to the various structures of the musculoskeletal system. By the end of the fourth week of gestation, a series of approximately 39 to 44 distinct cube-shaped bulges develop bilaterally within the mesodermal layer. These bulges are known as the mesodermal somites, and they divide the mesoderm into 44 segments (cranial to caudal).
As the nervous system develops further (from the ectoderm), a pair of nerve roots (spinal nerves) form adjacent to most of the original mesodermal somites. These nerve roots will eventually contain sensory, motor, and autonomic nerve fibers that will innervate skin, muscle, bone, and viscera. These connections give rise to the important concepts of dermatomes, myotomes, and sclerotomes (areas, respectively, of skin, muscle, and bone that are supplied by a single spinal nerve root). The skin of the posterior trunk retains most of the orderly innervation, originally derived in company with the 38 to 44 primitive segments. This gives rise to the notion that areas of skin on the posterior trunk have an embryonic link to various musculoskeletal and internal organs of the body (Head’s zones). Figure 11-1 illustrates this concept.
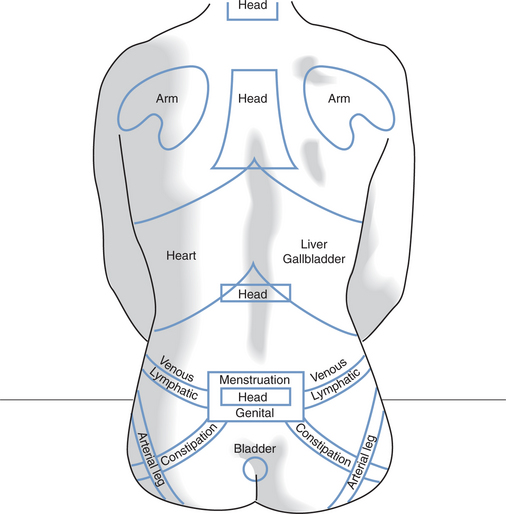
Figure 11-1 Body Areas (Head’s Zones) Represented on the Posterior Trunk
(Modified from Ebner M: Connective tissue massage: theory and therapeutic application, ed 2, Huntington, NY, 1985, Robert E Krieger.)
A key concept underpinning CTM and other systems involving manipulation of the soft tissues is that pathologic changes affecting any of the structures derived from a mesodermal somite eventually give rise to signs and symptoms in any related structures, especially in the skin and connective tissues. The fact that visceral lesions may give rise to changes in other areas is well known; for example, liver and gallbladder problems can be reflected in the right mid- to lower posterior costal segments (T6 to 10) and in the right upper rectus region. The changes that take place in a related zone are detectable by palpation of the skin and subcutaneous tissues of the same area. The connective tissues have characteristic areas of local tension. There is a certain tightness of the different layers against each other where normally there would be a limited amount of movement between them (Hirschberg, Fatt, & Brown, 1986). Within each zone of influence of a spinal segment or segments, there is often a circumscribed area that is related to a particular organ; these areas are known as maximal points. These changes can be detected by palpation of the area. Holey (1995a) and Holey and Watson (1995) described the basic concepts of zone recognition and inter-rater reliability in the detection of these zones.
A key treatment concept in CTM is the following:
The receptors are a wide variety of afferent endings in the skin, subcutaneous tissues, blood vessels, muscles, and the viscera. The effectors are largely smooth muscle fibers in a variety of tissues, such as blood vessels, viscera, glands, and the skin. The pathway is formed by the various interconnections between the afferent fibers of the somatic nervous system and the efferent fibers of the autonomic nervous system, especially through the sympathetic chain of the sympathetic division and the sacral outflow of the parasympathetic system. Figure 11-2 illustrates this concept.
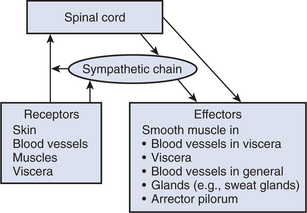
The autonomic reflex described previously connects the stimulation (including massage) of afferent receptors in the skin and subcutaneous tissue with potential responses in many different types of tissue. It is an important concept to help explain the mechanisms involved with the remote-site effects seen with CTM and other soft tissue manipulations. It is important to remember that the lumen of the small arterioles is largely under the control of sympathetic nerve fibers. When these fibers are active, they cause the smooth muscle in the arteriolar walls to contract, thereby producing vasoconstriction. When sympathetic fiber activity decreases, however, the smooth muscle relaxes and vasodilation occurs. This brings more blood, and therefore oxygen and nutrients, to the tissues. It also allows waste products from the tissue to be removed more efficiently. These effects are likely to facilitate healing in the tissues. It is also possible that a similar effect could be produced by a chemical rather than neural activation of autonomic reflex activity. Soft tissue manipulation could cause the local or general liberation of chemical substances that activate such a reflex. For example, vasoactive intestinal polypeptide (VIP) has a profound effect on the circulation and on systemic pain relief and has been associated with CTM (Kaada & Torsteinbo, 1987, 1989
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


