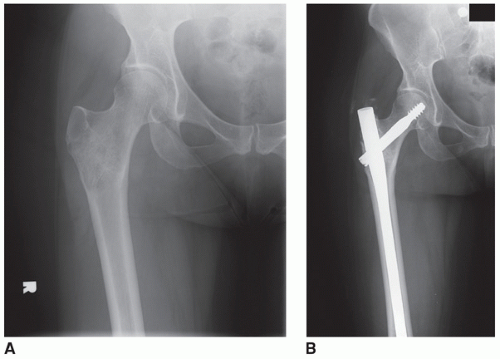
 FIGURE 13.1 Indications for stabilization must consider four factors: impending versus actual fracture, location, diagnosis, and prognosis. A: In this case, the patient had pain recalcitrant to medical management and irradiation associated with this mixed lytic/blastic intertrochanteric lesion from breast carcinoma. The patient was felt to have an impending pathologic femur fracture. B: Due to the intact bone and relatively good prognosis, the patient was treated with a third-generation femoral reconstruction nail (Long Gamma Nail, Stryker) locked proximally and distally. |
Location within the femur
Impending pathologic fractures
Femoral neck to distal femoral diaphysis
Rationale: If good bone stock remains in the femoral epiphysis to support the threaded portion of the reconstruction screw(s), an intramedullary reconstruction nail may still be utilized in this situation.
Key: Regardless of the location of the identifiable lesions, critically assess the remaining bone to ensure that adequate fixation is able to be achieved both proximal and distal to the lesion. Always have a backup plan.
Displaced pathologic fractures
Intertrochanteric region to distal femoral diaphysis
Rationale: Once a fracture has occurred, the femoral neck is no longer a reasonable option for consideration of the reconstruction intramedullary nail.
Key: Adequate bone stock proximal and distal to the fracture is necessary to obtain secure fixation.
Established diagnosis
Independent biopsy of the bone lesion directly at site of lesion and/or fracture prior to instrumentation of the intramedullary canal with guide rod, reamers, or nail
Rationale: Unless the patient already has well-established terminal metastatic disease with previously biopsy-proven metastatic lesions in bone, a biopsy will exclude the possibility of a sarcoma, a condition that should not be treated in most cases by intramedullary nailing.
Adequate life expectancy to expect benefits to outweigh risks
Medically fit to survive procedure and perioperative period
Rationale: While the mortality risk of a percutaneously inserted intramedullary nail is relatively small, patients who are immediately preterminal due to medical issues related to their cancer are best referred for hospice if they are unable to be optimized preoperatively.
Expected survival of 6 to 12 weeks minimum
Rationale: If patients are not expected to recover fully enough prior to their death to allow restoration of some function, the goals of the procedure are unlikely to be achieved.
More limited indications than third-generation reconstruction nail device
Requires solid bone immediately adjacent to bone lesion for secure fixation, a situation which is rare, as the region of poor bone quality may often be underestimated by the imaging studies
More prone to failure of internal fixation due to loss of secure purchase by screws in the bone
Fails to address presence and/or development of more distal bone lesions
Any anatomic site other than the intertrochanteric region
Presence of additional lesions elsewhere in the femur away from the intertrochanteric region that may develop problems if they progress
Inadequate proximal diaphyseal bone to provide secure screw fixation
TABLE 13.1 Contraindications and Alternative Surgical Options for Third-Generation Intramedullary Nail Fixation of the Femur | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
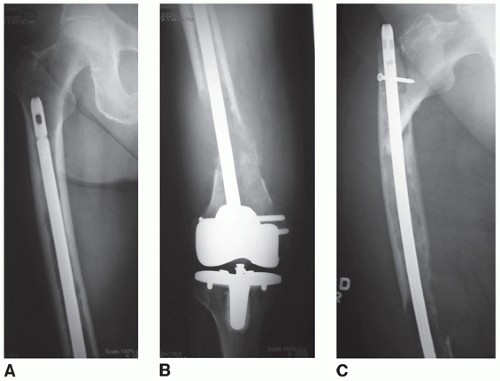 FIGURE 13.2 Retrograde femoral nails are not ideal for internal fixation of impending or actual pathologic femur fractures as they fail to adequately protect the proximal femur, a common site of bone metastases. This patient incurred a pathologic right distal femur fracture above a total knee arthroplasty. A,B. Biopsy showed metastatic carcinoma, and the patient underwent surgical stabilization utilizing a retrograde femoral intramedullary nail without bone cement supplementation. C: Subsequently the patient developed a second pathologic fracture through the proximal femur just above the retrograde femoral nail in the region left unprotected by the original stabilization. |
Confirm diagnosis
Preoperative metastatic workup to search for likely primary and identify extent of disease (if unknown)
Total skeleton bone scan
Computerized tomography of chest/abdomen/pelvis
Serum protein electrophoresis and urine protein electrophoresis to evaluate for multiple myeloma
Establish diagnosis of femoral lesion with tissue before proceeding with treatment (unless patient already has had tissue documentation of other bone metastases)
Preoperative needle biopsy
Intraoperative needle or open biopsy with frozen section
Assess extent of bone defect and remaining bone, proximal and distal
Plain biplanar radiographs of entire femur
Consider MRI or CT to assess extent of defect
Entertain alternative means of operative management
Consider alternatives if proximal (more likely) or distal bone proves inadequate to support fixation intraoperatively (Table 13.2)
Supplementation with bone cement
Proximal endoprosthetic device
Decide upon a backup plan and have implants available (see Table 13.2)
Ensure all equipment will be available
Primary plan: third-generation femoral reconstruction nail (or dynamic hip screw) of choice with insertion equipment, flexible intramedullary reamers and guide rod(s), radiolucent fluoroscopy table or fracture table, and c-arm fluoroscopy
Backup plan(s): bone cement with insertion device of choice (Toomey syringe), third-generation intramedullary reconstruction nail (if primary plan involves dynamic hip screw device), endoprostheses, and associated insertion equipment (see Table 13.2)
Consider preoperative embolization (Fig. 13.3)
Vascular malignancies: renal carcinoma, thyroid carcinoma, and myeloma
This is particularly important to consider for these techniques because whether the lesion is approached directly or indirectly (reaming through it), brisk bleeding may be encountered.
Tip of greater trochanter. Adequate access to the region proximal to the tip is crucial, so attention must be paid to this when placing the bump under the hip during positioning and also during draping.
Rotational landmarks: Anterior superior iliac spines, patella, and lateral femoral condyle should be assessed to ensure that postoperative rotation is optimal when dealing with displaced fractures.
TABLE 13.2 Reconstructive Alternatives to Internal Fixation Devices Based on Anatomic Region of Compromised Proximal Femoral Bone | ||||||||
|---|---|---|---|---|---|---|---|---|
|
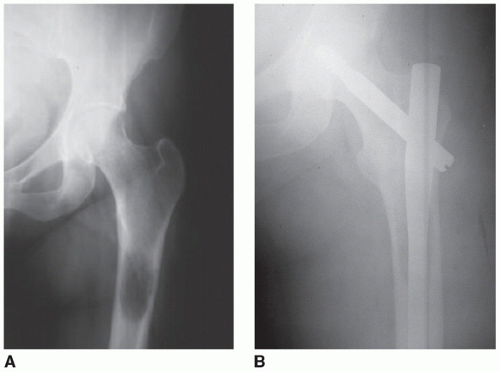 FIGURE 13.3 For metastatic lesions of the femur due to renal carcinoma, myeloma, or thyroid cancer, consideration should be given to preoperative embolization to minimize intraoperative bleeding. A: This patient with known metastatic thyroid cancer to the left femur subtrochanteric region with impending pathologic fracture had associated pain despite treatment with radioactive iodine. B: Considerable intraoperative bleeding was encountered during placement of this locked third-generation reconstruction nail (Long Gamma Nail, Stryker). |
To establish diagnosis. If a biopsy is to be done as part of the procedure, the approach should be from the lateral thigh directly at the site of the lesion, NOT through the intramedullary canal (Fig. 13.4C)! The frozen section diagnosis should be established unequivocally to be metastatic disease, myeloma, or lymphoma before proceeding to operative fixation. If there is a possibility that the diagnosis represents sarcoma, the procedure should be aborted until a definitive diagnosis is rendered on permanent sections.
For third-generation intramedullary nail insertion through the tip of the greater trochanter
Depending upon the size of the patient, the incision may vary from 2 to 6 cm.
Begin the incision at the center (anterior-posterior) of the tip of the greater trochanter and extend proximally.
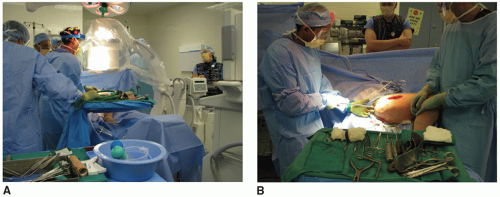 FIGURE 13.4 A: A typical intraoperative setup for femoral trochanteric nailing of an impending fracture is shown here. The patient is positioned on a radiolucent Jackson table to facilitate intraoperative imaging, the surgeon and assistants are on the operative side (patient’s right in this case), the fluoroscopy c-arm unit is coming in from the patient’s contralateral side (patient’s left in this case) to minimize interference with the use of instruments by the surgeon, and the viewing screen at the foot of the bed where it is unobstructed by other personnel or equipment. B: When there is no fracture, a fracture table is unnecessary, as in this case of an impending pathologic fracture. In a supine position with a bump under the operative hip to facilitate access to the trochanteric region, the operative limb may be easily manipulated to allow exposure to the lateral biopsy/curettage site (the larger midshaft incision in this case) as well as to the tip of the trochanter, as shown here for insertion of instruments and the implant into the femoral canal. The operative limb is adducted and internally rotated to bring the tip of the greater trochanter more anterior. In much the same manner, the limb can also be easily manipulated to obtain both anteroposterior and frog-lateral x-ray views with the fluoroscopy unit. This obviates the cumbersome and time-consuming rotation of the fluoro unit much of the time. |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


