Female Issues in Sport: Risk Factors and Prevention of ACL Injuries
Jeffrey R. Counts DO
Lori A. Bolgla PT, PhD, ATC
Mary Lloyd Ireland MD
Anterior cruciate ligament (ACL) injuries are becoming more common and costly.
The 15- to 45-year-old patient population is most likely to undergo an ACL reconstruction.
The main function of the ACL is to limit anterior tibial translation on the femur.
Although overall ACL injury rates for males and females are very similar, the rates do differ for specific sports. Studies have placed the rate of ACL injuries in female basketball players at 2.89 to 3.5 times higher than in males. The increased rate in female soccer players has been placed at 2.3 to 2.8 times that of males.
Mechanics appear to contribute significantly to the ACL gender bias. Females generally exhibit greater knee valgus, femoral internal rotation, and femoral adduction on an externally rotated knee. Proximal instability from the trunk and hip results in greater knee valgus and knee external rotation, postures known to place increased strain on the ACL. Trunk instability, combined with limited knee flexion, further increases the risk of ACL injury because smaller knee flexion angle limits the hamstrings’ ability to contract and prevent anterior tibial translation.
Females with either a lower extremity or low back dysfunction have demonstrated greater side-to-side hip extension strength symmetry than males.
Future studies should examine whether improvements in strength, proprioception, movement execution, or a specific combination of areas is most effective in preventing ACL injury. Those studies should also quantify the most appropriate time, duration, and intensity of participation in a prevention program relative to the competitive season.
Anterior cruciate ligament (ACL) injuries are one of the more serious injuries seen in sports medicine. Orthopaedic surgeons perform an estimated 100,000 ACL reconstructions (1) each year with an associated cost of approximately $1.7 billion (2). Furthermore, costs associated with conservative management of ACL injuries, postoperative rehabilitation, and long-term care of posttraumatic arthritis that may occur in certain situations further increase this financial burden. This has a huge economic impact. With today’s current emphasis on staying fit, statistics suggest that these numbers will continue to rise in the future. Daniel and Fritschy (3) have reported ACL injury rates of one per 3,500 enrollees across a large managed care–insured population. The 15- to 45-year-old patient population, which encompasses nearly 47% of the entire U.S. population, is most likely to undergo an ACL reconstruction. Griffin et al. (4) have reported ACL injury projection rates specific to this population as one per 1,750.
Nearly 70% of all ACL injuries occur during sports participation (3). Typically, males sustain a higher absolute number of ACL injuries because of their greater sports participation (3). Since the passage of Title IX in 1972, the number of females competing in organized sports has increased. Surprisingly, overall ACL injury rates for males and females are very similar (implying no gender differences). However, these rates do differ when looking at specific sports (5). The National Collegiate Athletic Association (NCAA) (6) has reported that female basketball players sustained an ACL injury at a rate 2.89 times higher than male basketball players, and others (7,8,9) have reported injury rates as much as 3.5 times higher for female basketball players. Female soccer players have incurred similar rates of injury, with their reported injury rates ranging from 2.3 to 2.8 times greater than male players (7,8,9).
TABLE 55-1 Summary of Factors Contributing to ACL Injuries | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||
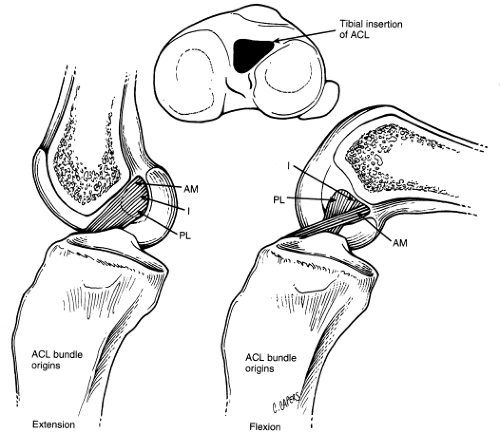 Fig 55-1. The anterior cruciate ligament (ACL) is divided into three bundles based on the tibial attachment: the anteromedial (AM), the intermediate (I), and the posterolateral (PL). With knee flexion, the posterior fibers loosen and the anteromedial fibers coil around the posterolateral ones. (From Baker CL, Flandry F, Henderson JM. The Hughston Clinic Sports Medicine Book. Baltimore: Williams & Wilkins; 1995. ) |
Basketball and soccer injuries usually result from a noncontact mechanism, which represents approximately 70% of all ACL injuries (4). Researchers (10) have described noncontact injuries occurring during two common movement patterns. First, injury may result during open cutting maneuvers. During the deceleration phase of a cutting maneuver, an athlete may exhibit an excessive knee valgus angle in combination with increased femoral internal rotation, resulting in an externally rotated knee. This combined loading has been shown to place a great amount of tension on the ACL that may lead to failure (11). ACL injury may also occur during the landing phase of a jumping maneuver
in which the athlete is in a relatively upright position with minimal hip and knee flexion. In this position, greater quadriceps and less hamstring activation increases the forward translation of the tibia on the femur, which may result in an ACL injury (12).
in which the athlete is in a relatively upright position with minimal hip and knee flexion. In this position, greater quadriceps and less hamstring activation increases the forward translation of the tibia on the femur, which may result in an ACL injury (12).
Several factors may contribute to noncontact ACL injuries and can be classified as being intrinsic or extrinsic (Table 55-1) (13). Intrinsic factors are structural and physiological in nature, representing those features that clinicians cannot modify. They include the intercondylar notch width, ACL size, absolute pelvic width, femoral length, physiological laxity, and hormonal influences. Extrinsic factors are those that can be modified with therapeutic interventions and include biomechanical and neuromuscular influences. In this chapter, we will explain how all of these factors may lead to injury and present prevention program strategies that may decrease the risk of ACL injury in the female athlete.
The ACL is an intra-articular, extrasynovial ligament that primarily restrains anterior tibial translation on the femur. The ligament passes through the intercondylar notch from an anteromedial to a posterolateral direction. The ligament has attachments along the posteromedial wall of the lateral femoral condyle and just anterior to the medial tibial eminence. It consists of two distinct bands, although a third intermediate band has also been described (14). These bands are defined based on their tibial attachments and consist of anteromedial and posterolateral bundles (Fig 55-1). As the knee moves, these bands provide differing stabilizing effects for the knee. When the knee is in full extension, the posterolateral bundle is tauter compared to the anteromedial bundle. As the knee flexes, the ACL assumes a relatively horizontal position. This position causes increased tightening of the anteromedial bundle and a loosening of the posterolateral bundle. One portion of the ACL remains under tension throughout the full range of motion, providing a continuous stabilizing effect for the knee.
ACL and Intercondylar Notch Size
Since 1938, researchers (15) have theorized that a smaller intercondylar notch size may increase the risk of ACL injury. They believed that ACL injury results from an increased stretch over the inner margins of the femoral condyles, which may occur at positions near full knee extension where the ACL can abut the roof of the intercondylar notch. Therefore, athletes who have a smaller sized notch may be more susceptible to an ACL injury because of the decreased space available within the intercondylar notch. Based on this relationship, researchers have investigated the correlation between intercondylar notch stenosis and ACL injury using plain radiographs, computed tomography (CT), and magnetic resonance imaging (MRI).
Plain Radiographs
Historically, physicians have assessed intercondylar notch size using plain radiographs. In an attempt to normalize notch size for comparison among subjects, Souryal et al. (16) developed the notch width index (NWI). This is defined as the ratio of the width of the intercondylar notch to the width of the distal femur at the level of the popliteal grove as seen on a tunnel view. They reported that high school athletes who sustained a noncontact injury had an NWI of 0.189 compared to 0.233 for those who injured their ACL during a contact mechanism. In a related study, Ireland et al. (17) reported that individuals who sustained an ACL injury had both smaller NWI and absolute notch width measurements, regardless of gender, than those individuals who did not injure their ACL ligament.
Researchers (18,19) have challenged the usefulness of the NWI. Shelbourne et al. (18) found that femoral bicondylar width increased as absolute femur length increased and believed that absolute notch width may be a more appropriate radiographic measurement. They reported a mean notch width of 16.9 mm and 14.5 mm, respectively, for noninjured males and females of similar height. For patients with unilateral ACL tears, the mean notch width decreased to 15.8 mm in males and 13.8 mm in females. The notch size decreased even more in those having bilateral ACL tears. For this subject cohort, males and females had average notch widths of 15.3 mm and 12.8 mm, respectively. Based on these findings, Shelbourne et al. (18) concluded that subjects with narrower absolute notch widths might possess a higher risk of injury.
Alternatively, others (20,21,22,23) have not found a relationship between notch size and incidence of ACL injury. The controversy in the literature may be due to limitations associated with plain radiographs that may influence measurement precision. Such factors include overlap and shadowing associated with plain radiographs and variation in knee position during radiography. Finally, plain radiographs only provide a two-dimensional view. Therefore, plain films may not adequately depict the true shape of the intercondylar notch and true relationship between the intercondylar notch and ACL size.
CT and MRI
More recently, researchers have analyzed the three-dimensional features of the intercondylar notch using more advanced imaging technology. Anderson et al. (24) collected CT images of the distal femur, created composite drawings of the intercondylar notch, and consistently identified five general shapes. Shapes ranged from an inverted “U” to a crested wave–shaped notch with a flattened superior medial
corner. The crested wave shape resulted in a more stenotic notch. Patients with this morphology had a higher incidence of ACL injury, regardless of gender.
corner. The crested wave shape resulted in a more stenotic notch. Patients with this morphology had a higher incidence of ACL injury, regardless of gender.
MRI has also been used to study the size of the intercondylar notch and the ACL. Davis et al. (25) reported a positive correlation between absolute intercondylar notch and ACL width. They also found that males exhibited larger notch and ACL widths than females. Other researchers have also compared ACL cross-sectional area between genders (19,26). In these studies, they reported larger ligaments in male subjects. They inferred that a smaller ligament may be weaker and more vulnerable to forces generated during certain athletic maneuvers. Some researchers have examined the strength of different sized ACL specimens and reported that a 14-mm ligament may withstand loads of up to 2,900 newtons (N), whereas a 10-mm ligament can only withstand loads up to 2,070 N (27). Few studies have examined this relationship, and more are needed to establish the relationship between ACL size and ligamentous strength.
Structural Alignment
Studies have shown that females tend to perform running and cutting activities with greater valgus angles and external abduction moments of the knee compared to males. Fung and Zhang (11) have shown that these actions may place greater strain on the ACL, and researchers have studied gender differences related to structural alignment. They have theorized that the structural malalignment that contributes to these movement patterns may increase the risk of ACL injury in the female athlete.
Conventional wisdom suggests that females have wider pelvises, which may lead to coxa varum, genu valgus, and increased rotational forces at the tibiofemoral joint. However, a study by Horton and Hall (28) found that, in absolute terms, females had smaller pelvic widths compared to male subjects. Subsequently, Livingston and Gahagan (29) examined pelvic width by calculating a hip width to femoral length ratio for males and females. Although females had smaller absolute pelvic widths, their hip width to femoral length was greater than in males. These authors concluded that the shorter femur length associated with female subjects increased the hip adduction required to position the feet under the center of mass of the body. This, in turn, may increase the knee valgus angle and, perhaps, the strain on the ACL. Therefore, the pelvic width to femoral length ratio might be more predictive of ACL injury than absolute pelvic width alone.
Loudon et al. (30) studied static structural faults that may be predictive of ACL injury. They reported that knee hyperextension, excessive navicular drop, and excessive subtalar joint pronation discriminated between females with and without ACL injury. They also determined that the presence of two or more structural faults may be more predictive of ACL injury than any one alone. For example, knee hyperextension in combination with tibial internal rotation can stretch the ACL over the lateral femoral condyle. During weight-bearing activities, subtalar pronation is coupled with tibial internal rotation (31). Therefore, excessive pronation can impart additional strain to the ACL, making it more vulnerable to injury. However, this study was retrospective in nature; it is unknown if these factors conclusively caused the ACL injury.
Tibial Plateau Orientation
The posterior slope of the tibial plateau has been suggested to contribute to ACL injury risk. This angle is formed by the tibial plateau in relation to the long axis of the tibia. The normal posterior slope ranges from 10 to 12 degrees. However, a steeper posterior slope may increase anterior tibial translation by placing the femur in a more posteriorly directed position relative to the tibia. Dejour and Bonnin (32) measured tibial slope and anterior tibial translation, using the radiological Lachman test, for the involved and uninvolved knee in subjects having a unilateral chronic ACL rupture. They then used linear regression analysis to determine the relationship between anterior translation and tibial slope. This analysis showed a 3.5-mm increase of anterior tibial translation for every 10-degree increase in tibial slope, and it was thought that a higher tibial slope may contribute to ACL injury. However, Meister et al. (33) measured posterior tibial slope in subjects diagnosed with and without ACL injury. Their results did not find differences in tibial slope between groups and were unable to validate this as a risk factor associated with ACL injury. Because limited research exists in this area, future investigations are needed to establish the possible relationship between tibial plateau orientation and ACL injury.
Physiological Laxity
The main function of the ACL is to limit anterior translation of the tibia on the femur. Failure occurs when the anterior load exceeds the strength of the ligament. Some researchers (34,35) have suggested that increased joint laxity results in excessive anterior tibial translation and ACL injury. Therefore, there has been some focus on the influence of both generalized joint laxity and ligamentous laxity on ACL injury.
Nicholas (36) originally reported a relationship between generalized joint laxity and knee injury in male football players. These relationships have also been compared between males and females in the context of understanding the gender bias in ACL injuries. Both Ostenberg and Roos (37) and Soderman et al. (38) have found generalized joint laxity to be a significant factor in the gender bias for ACL injury.
The KT-1000 Ligament Arthrometer (Med-Metric, San Diego, CA) has been used to assess gender differences in ligamentous laxity. Prior work has shown that collegiate female athletes have greater anterior tibial translation than their male counterparts (39,40,41). Furthermore, Uhorchack et al. (42) reported that females who exhibited ligamentous laxity values of one or more standard deviations above the mean were 2.7 times more likely to sustain a noncontact ACL
injury than those with less laxity. This ligamentous laxity, in combination with a decreased intercondylar notch size, may further increase the likelihood of sustaining an ACL injury.
injury than those with less laxity. This ligamentous laxity, in combination with a decreased intercondylar notch size, may further increase the likelihood of sustaining an ACL injury.
Related posts:
 Periarticular Ligamentous Tissue: A Biochemical and Physiologic Assessment
Functional Spinal Rehabilitation
Acute Injuries: Shoulder Fractures and Acromioclavicular and Sternoclavicular Joint Injuries
Hip Arthroscopy
Medial Collateral Ligament
Anatomic Double Bundle Anterior Cruciate Ligament Reconstruction
Periarticular Ligamentous Tissue: A Biochemical and Physiologic Assessment
Functional Spinal Rehabilitation
Acute Injuries: Shoulder Fractures and Acromioclavicular and Sternoclavicular Joint Injuries
Hip Arthroscopy
Medial Collateral Ligament
Anatomic Double Bundle Anterior Cruciate Ligament Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


