F
facial injury injuries to the structures in and around the face including the facial bones; abrasions and lacerations, septal and auricular haematomas and other injuries around the nose, ears and eyes. Sport accounts for up to 25% of facial injuries. They can result from direct contact with another person, with equipment such as a squash racquet, a goalpost or the ground. Common in contact sports such as rugby and boxing. The incidence can be reduced by the use of protective equipment, e.g. hockey goalkeeper’s face protector.
falsificationism view, propounded by the philosopher Popper and coming to prominence in the English-speaking world in the 1950s, that the hallmark of good science is to challenge every hypothesis or theory (‘conjecture’) by actively identifying and testing predictions which follow only from it, not from competing theories, one criterion of a good theory being that it gives rise to many such explicit, unique and so ‘vulnerable’ predictions. Failure of the prediction will then falsify or refute the theory; on the other hand, success of a prediction can be regarded as corroborating evidence but not as irrefutable proof, which is never possible. aka refutationism; contrasts with verificationism.
fast muscle fibres see muscle fibre types.
fat true or neutral fats belong to the broad category of lipids; they consist of one molecule of glycerol combined with three fatty acids to form a triglyceride (syn triacylglycerol). dietary fat may be of animal or vegetable origin. Vegetable fats with polyunsaturated and monounsaturated fatty acids are liquids (oils) whereas the animal fats, e.g. on a lamb chop, contain more saturated fatty acids and are solid. ‘Fats’ is sometimes used loosely to include other lipids. See also body fat.
fat-free (body) mass (FFBM/FFM) see body composition.
fatigue reduction in ability to sustain a physical or mental function as a consequence of the intensity and/or duration of the effort. Fatigue can last for periods ranging from a few tens of seconds to several days, its duration broadly correlating with that of the fatiguing activity, e.g. recovery from a 60 m sprint takes only a few minutes but few people would wish to run competitive marathons less than 7–10 days apart. See also central fatigue, glycogen, muscle fatigue.
fatty acids the main components of fat, consisting of straight hydrocarbon chains with the number of carbon atoms ranging from 4 to more than 20, although chains of 16 and 18 are the most prevalent. All fat-containing foods, and all fat or lipid in the human body, consist of a mixture of different proportions of (1) saturated fatty acids (SFA) which have only single bonds between carbon atoms, all the remaining bonds being attached to hydrogen. SFA occur primarily in animal products like beef, lamb, pork, chicken, cream, milk, butter. Coconut and palm oil, hydrogenated margarine, commercially prepared cakes, pies, and biscuits are also rich in SFA; (2) monounsaturated fatty acids (MUFA) which have one double bond along the main carbon chain. They are present in canola oil, olive oil, peanut oil and oil in almonds, pecans and avocados; (3) polyunsaturated fatty acids (PUFA) which have two or more double bonds along the main carbon chain. Safflower, sunflower, soybean and corn oil are rich in PUFA. See also essential fatty acids, free fatty acids, omega-3 fatty acids.
female athletic triad the combination of an eating disorder, amenorrhoea and osteoporosis. The signs may be hidden by the athlete, making the diagnosis difficult, though early recognition can be achieved through risk factor assessment and screening questions. Risk factors include being a competitive athlete, taking part in sports in which low body weight is an advantage (such as gymnastics) or endurance sports (such as distance running). More common in those whose sport takes up all of their free time, and who may be under pressure from parents or coach. Features include amenorrhoea for more than 3 months, fainting, loss of weight to more than 10% below ideal. Decreased bone mineral density can result in recurrent premature osteoporotic stress fractures, with normal density never regained. There is also low self-esteem, anxiety, excessive exercise and a preoccupation with food and weight management. Treatment requires involvement of the athlete, her parents, coach, doctor and nutritionist, and includes appropriate diet, exercise modification and psychological support and counselling.
femoral referring to the thigh.
femur the thigh bone – the longest and strongest in the body. Articulates proximally with the pelvis at the hip and distally with the tibia at the knee. Fractures of the femur can result in significant blood loss and clinical shock. See appendix 1.2 figs 1, 2.
ferritin an iron-protein complex, which acts as a store for iron. Found mainly in the liver but also in the spleen and bone marrow. Serum ferritin measurement is used as a marker of total body iron. See also anaemia.
fibre see connective tissue, muscle fibre, nerve fibre, non-starch polysaccharides.
fibrillation unco-ordinated contraction of muscle, referring usually to heart muscle. atrial fibrillation chaotic atrial rhythm with irregular transmission to the ventricles, causing irregular heart beat. ventricular fibrillation ineffective ventricular activity with failure of cardiac output. A common cause of sudden death following myocardial infarction.
fibula (Latin clasp) the smaller and outer of the two bones of the lower leg; articulates with the lateral condyle of the tibia at its upper end, and with the tibia and talus at its lower end. It is non-weight-bearing but assists in stabilizing the ankle. See appendix 1.2 fig 1.
finger injury see dislocation, mallet finger, trigger finger.
fitness test test performed to assess an individual’s physical ability to undertake a specific activity, e.g. after recovery from injury.
flexibility the range of movement around a joint; dependent on a number of factors, including the size and shape of the bones, the ability of tendons to stretch, the condition of the ligaments, normal joint mechanics, soft tissue mobility and extensibility of the muscles. Good flexibility is beneficial in sport especially, for example, gymnastics and should be part of a sports-specific training programme and warm-up. However, flexibility training needs to be balanced with strength training to maintain joint stability. flexibility assessment can be made directly by measuring the angle of joint displacement using a goniometer, but this requires a skilful operator to achieve consistent results. More indirect measurements include the sit-and-reach or standing toe-touch tests. See also hypermobility.
flexion a movement which decreases the joint angle between two ventral surfaces of the body, e.g. bending the elbow or knee, tilting the head forwards. flexor muscles those with this action, e.g. biceps, hamstrings. Opposite of extension. See appendix 1.2 fig 3.
flow (1) the volume of a fluid (liquid or gas) moving per unit time, e.g. blood flow to or through a region of the body, expressed in mL per minute; (2) in psychology, a state of complete involvement and focus on a task that occurs when there is a perfect match between one’s skills and the demands of the task.
flow-volume loops graphical representation of the relation between inspiratory and expiratory airflow and the change in volume of the lungs; used in the assessment of lung function with respect to patency or obstruction of the airways, e.g. in the assessment of asthma.
fluid balance see hydration status, water balance.
fluid dynamics the study of motion (strictly accelerating motion) in or of a fluid medium (liquid or gas).
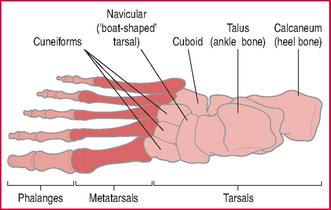
foot as well as supporting the weight of the body, the foot works as a lever to move the body forwards. The many joints between the bones of the foot allow it to change shape to accommodate different and uneven surfaces. The skeleton of the foot consists of: the seven tarsal bones, including the heel bone (calcaneum) and the talus which articulates with the leg bones at the ankle joint; beyond these, the five metatarsals and, in the toes, the phalanges. There are layers of small muscles in the sole, and tendons from the lower leg traverse the ankle to reach their various insertions in the sole and on the dorsum (upper part) of the foot. See appendix 1.2 fig 6.
< div class='tao-gold-member'>