22 Examination of varicose veins



Introduction
The type of examination may not be immediately obvious if an examiner asks a student to ‘examine this patient’s legs’. The patient may be lying, sitting or standing. Once both the patient’s legs are fully exposed, they should be examined for signs of varicose veins and chronic venous insufficiency (below), arterial ulcers and gangrene (Ch. 28), swollen/deformed joints (Charcot’s joints; Ch. 28) and wasting (neurological, a medical issue).
Inspection
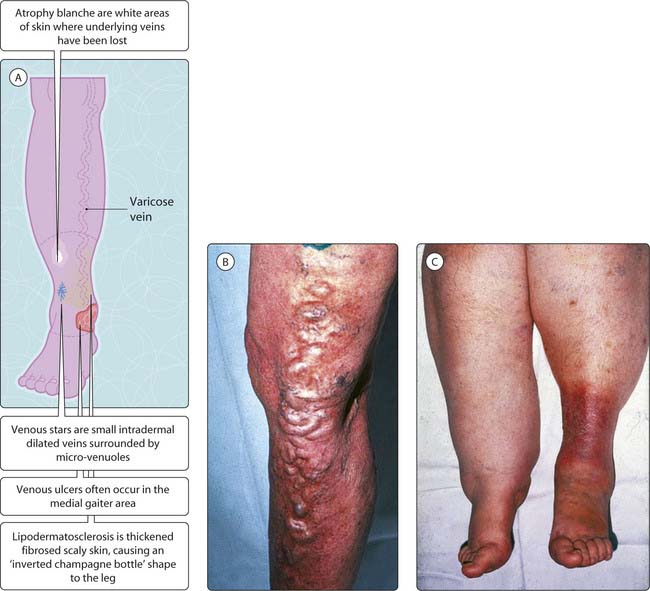
You may be asked only to make a visual inspection and talk about what you see, and not necessarily touch the limb. For varicose veins, it is necessary to identify which vein is affected and where the level of incompetence is. Inspect the legs while the patient is standing up with both legs fully exposed. Varicose veins have a dilated, tortuous course and this should be described (Fig. 3.22.1). The long saphenous vein is involved in most cases; it runs anterior to the medial malleolus and up the medial aspect of the calf, knee and thigh to drain into the saphenofemoral junction. The short saphenous vein is involved less often; it runs from the lateral aspect of the calf and into the popliteal fossa, to drain into the saphenopopliteal junction. Other features (Fig. 3.22.1A) can be remembered by the acronym VVV LAPS: varicose veins, venous ulcers, venous stars, lipodermatosclerosis, atrophy blanche, pitting oedema and scars (both groins and both legs may have scars of previous operations). Patients may have simple and solitary varicose veins, some of the features of chronic venous insufficiency or all of the features (indicating severe disease).
< div class='tao-gold-member'>




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


