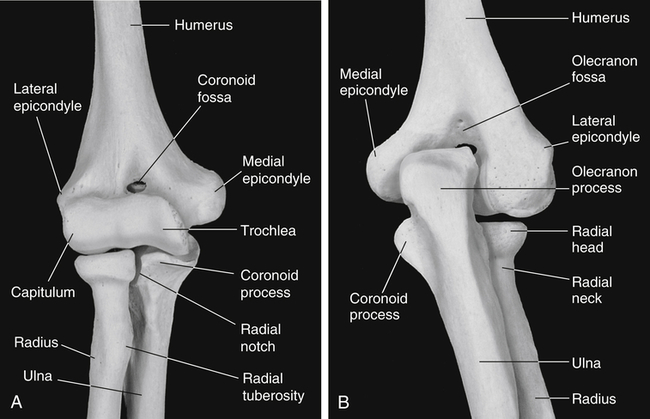
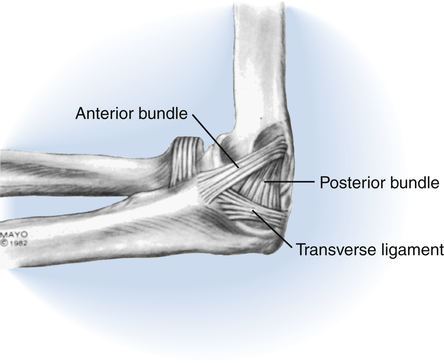
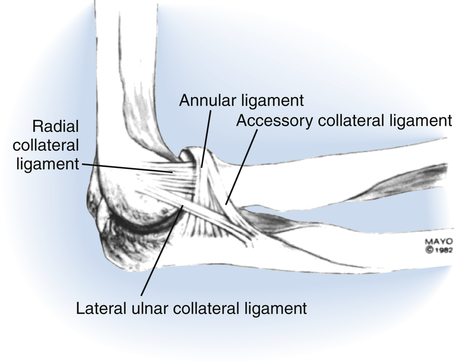
The elbow serves as the essential functional link between the hand and the shoulder, allowing the hand to be brought inward toward the body and outward into the surrounding environment. It also transfers force through the upper extremity (UE) during weight bearing on the hand. The functional range of motion (ROM) required at the elbow is reported to be 30° of extension, 130° of flexion, and 50° each of pronation and supination.1 However, because functional demands vary, the range required will differ somewhat among individuals. In general, it is easier to compensate for limited extension by moving closer to objects during reach than it is to compensate for limited flexion. Because the most common complication of elbow trauma is stiffness, it is essential that therapists treating individuals with elbow injuries be well versed in effective treatment approaches. To “push harder” or “be more aggressive” is not an effective solution and may instead cause more damage and stiffness. In addition to being mobile, the elbow must also be stable so that it can withstand the forces of daily activities. Maintaining the most effective balance between minimizing stiffness through early motion, preserving stability, and protecting healing structures is a challenge even for experienced therapists. Three bones contribute to the elbow joint, the distal humerus, proximal ulna, and proximal radius (Fig. 23-1). They form the three articulations of the elbow: the ulnohumeral, radiohumeral, and proximal radioulnar joints. The distal humerus has two articular surfaces: the spool-shaped trochlea medially and the convex capitellum (also known as the capitulum) laterally. The ulnohumeral joint is the close articulation of the trochlea with the rounded trochlear notch formed by the coronoid and olecranon of the proximal ulna. In full elbow flexion the coronoid fossa on the anterior distal humerus receives the coronoid process of the anterior trochlear notch. In full extension, the olecranon fossa on the posterior distal humerus receives the olecranon process of the posterior trochlear notch. The radiohumeral joint is the articulation of the capitellum of the distal humerus with the shallow concavity on the proximal aspect of the radial head. The radial head and the radial notch of the ulna form the proximal radioulnar joint. Due to the oblique orientation of the trochlea of the humerus, in full extension the elbow has a valgus angle, known as the carrying angle. It has been widely reported that men have a carrying angle of approximately 5° to 10°, while women have a slightly greater carrying angle of approximately 10° to 15°. However, measured radiographically, the normal carrying angle in adults is reported to be 17.8° on average with no significant difference between men and women.2 The three elbow articulations share a common joint capsule. The medial and lateral collateral ligament complexes of the elbow are essentially thickenings of the joint capsule. Portions of the collateral ligament complexes remain taut throughout elbow flexion and extension, making an essential contribution to static elbow stability. The medial collateral ligament complex (Fig. 23-2) has three components, the anterior bundle, posterior bundle, and the transverse ligament. This ligament complex, particularly the anterior bundle, stabilizes the elbow against valgus (abduction) forces. The lateral collateral ligament complex (Fig. 23-3) has four components, the lateral ulnar collateral ligament (LUCL), the radial collateral ligament, the annular ligament, and the accessory lateral collateral ligament. The lateral collateral ligament complex is considered to be one of the primary stabilizers of the elbow. It provides restraint from varus (adduction) forces. The LUCL, one of the four components of this ligament complex, also provides posterolateral stability to the ulnohumeral joint. Edema often affects all three joints of the elbow because they share a common joint capsule. Fractures of the distal humerus are relatively uncommon, accounting for only 2% of all fractures. They occur most frequently in young males and in females over 80 years of age. In younger individuals, distal humeral fractures are usually associated with higher velocity injuries, such as motor vehicle and sports-related accidents. In the elderly with poor bone stock, they can occur from a simple fall onto an outstretched hand.3 Displaced radial head fractures with comminution or mechanical block to forearm rotation require operative treatment. The presence of one or more associated injuries at the elbow including capitellum fracture, olecranon fracture, ligamentous injuries, and elbow dislocation, is also an indication for operative treatment. Approximately one in three radial head fractures is associated with another injury.4 Options for the operative treatment of radial head fractures include internal fixation with plate and screws, radial head excision, and radial head replacement. Comminuted fractures are treated with radial head excision or replacement. Displaced fractures with mechanical block to forearm rotation are treated with internal fixation or radial head excision. Note that due to important stabilizing function of the radial head, it must be replaced rather than excised in radial head fractures with associated injuries that compromise elbow stability. Most olecranon fractures require open reduction and internal fixation. A posterior approach is typically used. The type of internal fixation is chosen depending on the individual characteristics of the fracture. Options include Kirschner wires, tension band wiring, compression screws, and plate fixation. With appropriate management, outcomes of olecranon fractures are typically good to excellent.5 In addition to the complications common to all elbow fractures, hardware on the posterior aspect of the elbow is not always well tolerated. Chronic irritation can result in olecranon bursitis and may require excision of the hardware.6 Distal humeral fractures that are comminuted, displaced, involve the trochlea or capitellum, or have neurovascular involvement require operative treatment. There is a higher risk of complications in high-energy mechanisms of injury, open fractures, and non-operatively managed fractures. In addition to the complications common to all elbow fractures, heterotopic ossification, bone in nonosseous tissues, may develop following fractures of the distal humerus. Although these fractures are frequently challenging to manage, the majority heal within 12 weeks without significant complications.3 Most are stabilized surgically with open reduction and internal fixation with plates and screws. A posterior surgical approach is most commonly used for visualization of the fracture. The triceps is split or elevated and reflected, or an olecranon osteotomy is performed. Following an olecranon osteotomy, the olecranon is reattached with Kirschner wires and screws or plating.7 An anterior ulnar nerve transposition is sometimes performed during surgery for fracture repair to lessen the likelihood of postoperative ulnar neuropathy. Elderly individuals with complex distal humerus fractures and osteoporotic bone present a particular challenge to the surgeon. Total elbow arthoplasty may be necessary in these individuals if screws cannot obtain adequate bony purchase for fracture fixation.8 • Which bone was fractured, and what was the nature of the fracture? Ask for the radiology report. • Were there any associated injuries? • Was the fracture treated surgically, and if so, how? Ask for the operative note. • Is the fracture stable enough to begin active motion? • Are there any movement limitations or other precautions? • What are the preferred type, position, and wearing schedule for the protective orthosis? Radial head fractures that are non-displaced or minimally displaced are treated non-operatively, unless there is a mechanical block to forearm rotation. These fractures have a favorable prognosis as long as motion is begun early. Active motion is usually initiated within the first several days following injury. Be sure to emphasize elbow extension, because this motion is most frequently lost after radial head fracture. Immediate mobilization has been shown to result in less pain and better elbow function at 1-week follow-up as compared to motion initiated 5 days following radial head fracture; although results were similar with respect to pain, ROM, and function at 4-week follow-up.9 Non-displaced and minimally displaced radial head fractures treated non-operatively do not require as long of a period of protective immobilization as other elbow fractures and radial head fractures treated operatively. The use of a sling or orthosis for comfort during the first week is usually sufficient. Not all individuals with non-operatively managed radial head fractures require repeated therapy visits to achieve good results. However, to minimize the risk of elbow flexion contracture, it is important to provide a structured therapy program to individuals who are reluctant to move or who are stiff after several weeks of performing a home exercise program. Most distal humeral fractures require operative treatment. However, some non-comminuted, stable fractures with minimal or no displacement can be treated with closed reduction followed by immobilization in a cast or orthosis. To minimize the risk of stiffness, gentle motion must be started after no more than 2 weeks of full-time mobilization. If the distal humerus is not stable enough to tolerate motion after this period of initial immobilization, it is best treated surgically to achieve the necessarily stability to allow early motion.6 When treating a patient referred to you following surgery for a distal humerus fracture, initiate elbow motion exercises with passive or gravity-assisted extension and active flexion. Depending on the type of surgical exposure that was used, either the triceps mechanism or the olecranon osteotomy may require protection for the first 6 weeks or so. Therefore, check with the surgeon before beginning active elbow extension and passive elbow flexion. • You will usually fabricate a thermoplastic posterior elbow orthosis to provide protection and support to the recently fractured elbow. Braces, casts, and slings are sometimes used as alternatives to orthoses. • Most isolated elbow fractures are immobilized with the elbow in 90° of flexion with the forearm in neutral rotation. Olecranon fractures that are managed non-operatively or have tenuous fracture fixation may require immobilization in more extension to minimize the pull of the triceps at its insertion on the olecranon. • Instruct your patient to remove the orthosis several times daily for active motion exercises unless contraindicated due to instability. Daily removal of the orthosis for hygiene is usually permissible, although initially wearing it covered with a plastic bag or cast cover while showering or bathing offers greater protection. • Even with optimal treatment, regaining full or at least functional motion following elbow fracture can be challenging. If your patient’s elbow motion plateaus, fabricate or provide a static progressive or serial static orthosis once the fracture has healed sufficiently (see “The Stiff Elbow” section). • Unless contraindicated, it is often most comfortable for your patient to begin elbow flexion and extension in supine with the upper arm supported on a pillow or folded towel alongside their torso. Progress to other gravity-assisted positions, such as elbow extension while seated and elbow flexion in supine with the shoulder flexed at 90°. • Instruct your patient to gently support the involved UE with their uninvolved hand while performing gentle motion exercises to increase comfort and control. • It is common to compensate for limited forearm ROM by leaning to the side or substituting shoulder motion. Minimize this by having your patient support the upper arm against their torso while they pronate and supinate the forearm. Maintaining erect posture may be easier initially if forearm rotation is performed bilaterally. • Longer holds at end range are more effective for increasing motion than performing a greater number of fast repetitions. • An early means of increasing motion is through active-assisted “place and hold” exercises in which the joint is placed at its end range position followed by an active holding of the position. • Precondition soft tissues with moist heat to make active and passive motion exercises more comfortable and effective. • When the physician determines that there has been sufficient fracture healing, begin strengthening with isometric exercises and progress to isotonic exercises. In addition to addressing strength deficits of triceps and the elbow flexors, also address any strength deficits of the shoulder girdle, shoulder, wrist, and hand. • Be sure not to overlook triceps, which tend to be weak following elbow injury. An effective exercise for initiating activation and strengthening of the triceps is elbow extension in supine with the shoulder flexed at 90°. • Adhere to precautions related to your patient’s fracture, surgery, and phase of healing, and be sure that your patient understands them. Don’t sacrifice stability for the sake of mobility. • Progress treatment based on the healing of your patient’s fracture as determined by their referring physician and on their individual response to therapy. • Passive motion and stretching should be performed slowly and gently. Forceful passive motion may damage rather than lengthen soft tissues. • Be alert for symptoms of ulnar neuritis, such as numbness or tingling in the small finger and ulnar aspect of the ring finger, and if present, report them to the referring physician.
Elbow Diagnoses
Function of the Elbow
Elbow Anatomy
Ligaments
 Clinical Pearl
Clinical Pearl
Elbow Fractures
Distal Humeral Fractures
Operative Treatment
 Questions to Discuss with the Physician
Questions to Discuss with the Physician
Diagnosis-Specific Information That Affects Clinical Reasoning
 Tips from the Field
Tips from the Field
 Precautions and Concerns
Precautions and Concerns
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Elbow Diagnoses
 Clinical Pearl
Clinical Pearl Clinical Pearl
Clinical Pearl Clinical Pearl
Clinical Pearl Clinical Pearl
Clinical Pearl Clinical Pearl
Clinical Pearl Clinical Pearl
Clinical Pearl What to Say to Clients
What to Say to Clients Clinical Pearl
Clinical Pearl Clinical Pearl
Clinical Pearl
