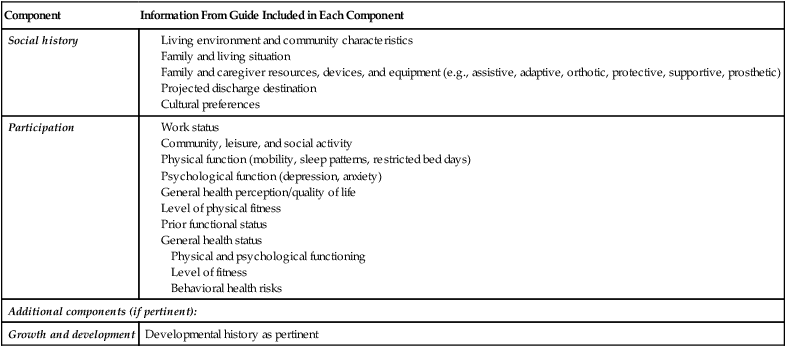
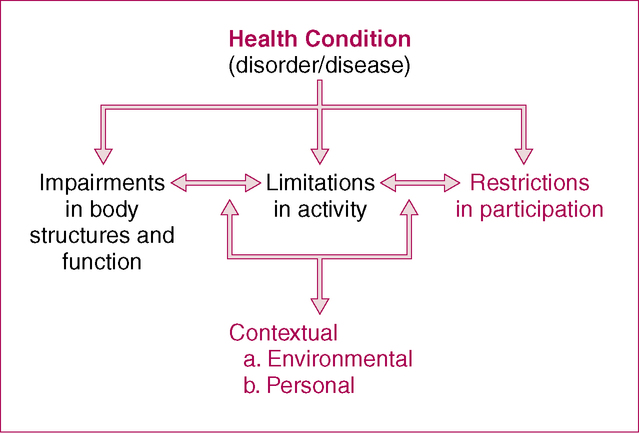
After reading this chapter and completing the exercises, the reader will be able to: 1. Describe the components of documenting participation, social history, and general health status. 2. Describe the usefulness of standardized outcome measures for documenting participation. 3. Describe the process of conducting an interview to obtain information pertaining to level of participation, social history, and general health status. Chapter 5 discussed documentation of reason for referral as it pertains to medical information and health condition. A second important part of documenting reason for referral relates to social history and participation (Figure 6-1). This addresses both environmental and contextual factors and describes the ability of a patient or client to perform the specific functions pertinent to his or her everyday life. How is the current condition affecting the individual’s life? What are the patient’s current life roles, and is the patient able to perform his or her roles as a husband/wife or father/mother? What is the person’s home and/or work environment, and how does it affect his or her ability to function independently? Can he or she work in either a paid or volunteer position? Is he or she able to engage in social and recreational activities? Assessment of participation clearly sets the rehabilitation professional apart from many other medical professionals. Medical doctors, for example, spend much of their time determining an accurate health condition and relating the patient’s impairments to that condition. Conversely, PTs should (and often do) spend a significant amount of their time at the other end of the disability spectrum—focusing on the interrelationship between participation and activities and between activities and impairments. Obtaining this information that encompasses a patient’s specific life roles provides the foundation for shaping the rehabilitation process. As noted in Chapter 1, it is the starting point for the process of rehabilitation. The Guide to Physical Therapist Practice (APTA, 2001) outlines various aspects of patient history taking that are part of the examination process. Table 6-1 details aspects of the patient history that can be categorized in this section of a note. Depending on the patient’s problems and length of the evaluation, each component can be documented independently (Case Examples 6-1 and 6-2) or generally combined (Case Example 6-3). The degree to which the headings Participation and Social History are used may differ depending on the institution and patient population. In addition, other information can be included here. General Health Status is often included in this section and includes information pertaining to the patient’s overall health and wellness. This information could include physical and psychological functioning, level of fitness, and behavioral health risks (e.g., history of smoking) or growth and development (in pediatric cases, e.g., date at which child began sitting or walking). Case Examples 6-1 through 6-3 provide sample documentation of participation and social history in different clinical settings (also see Case Examples 4-1 to 4-4). TABLE 6-1 Components of Documenting Reason for Referral: Participation and Social History This table incorporates terminology found in American Physical Therapy Association: The guide to physical therapist practice, ed 2, Alexandria, VA, 2001, American Physical Therapy Association, p S36.
Documenting Reason for Referral
Participation and Social History
Components of Documenting Participation and Social History
Component
Information From Guide Included in Each Component
Social history
Participation
Additional components (if pertinent):
Growth and development
Developmental history as pertinent
< div class='tao-gold-member'>
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


