Chapter 26. Disorders of the spine
Cervical spine
Acute disc prolapse
The cervical spine is very flexible and the intervertebral discs are subjected to considerable strains. The cervical roots cross the discs as they leave the spinal canal, where they are vulnerable to pressure from disc protrusion (Fig. 26.1). Disc protrusions in the neck are usually more lateral than those in the lumbar spine and affect one level only.
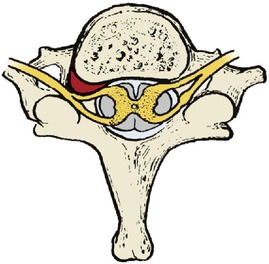 |
| Fig. 26.1 Cervical disc protrusion compressing a cervical root. |
As in the lumbar spine, disc protrusions are accompanied by pain, altered sensibility and weakness. The four lowest roots are most often affected and are accompanied by pain and sensory symptoms in the radial side of the forearm and hand, with weakness of grip (C8) and elbow flexion (C5–6).
Movement of the cervical spine is also restricted, particularly flexion and rotation on the affected side.
Treatment
Conservative treatment. Analgesics, rest, a collar and traction will usually produce a remission of symptoms but the pain may be so severe and intractable that disc excision is required as an urgent procedure.
Operative treatment. Disc excision may relieve pain and improve neurological function but it makes the cervical spine more unstable than the corresponding operation on the lumbar spine and the root can still be irritated even when the disc has been excised. To avoid this, operation is sometimes accompanied by a cervical fusion in which a block of bone is inserted between the adjacent vertebral bodies. The role of cervical fusion, which puts greater strain on the intact discs, is controversial.
Cervical spondylosis
Cervical and lumbar spondylosis are almost universal in patients over the age of 40 but seldom cause symptoms.
Spondylosis is different from osteoarthritis because it occurs around intervertebral discs instead of in synovial joints (Fig. 26.2). The posterior facet joints are synovial joints and may develop osteoarthritis but the cartilage joints between the vertebrae cannot do so because they have no joint space. For practical purposes, however, the two conditions can be considered together and treated as degenerative joint disease.
 |
| Fig. 26.2 Cervical spondylosis. The patient also has congenital fusion of C2 and C3. |
Patients with cervical spondylosis feel a dull pain in the neck radiating across the shoulders and down the upper part of the arm, worse on movement. The pain can be confused with supraspinatus tendinitis and other shoulder disorders.
Treatment
The standard treatment consists of heat, rest, anti-inflammatory drugs, analgesics and a supporting collar. When the symptoms have subsided, mobilizing exercises to restore movement are important but it must be said that no properly conducted scientific study has ever shown that these exercises influence the natural history of the disease. Voltaire may have been right when he commented that ‘The efficient physician is the man who successfully amuses his patients while Nature effects a cure’.
Operation is seldom required for spondylosis but may be necessary if there is severe pain arising from a single identifiable level (Fig. 26.3).
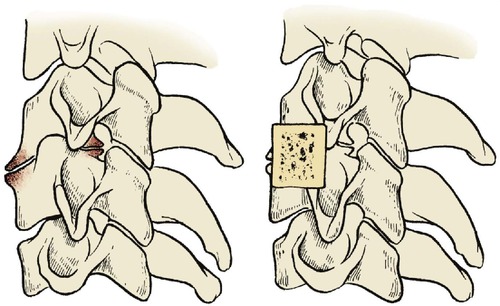 |
| Fig. 26.3 Cervical fusion. A bone block prevents movement and holds the affected vertebrae apart. |
Rheumatoid arthritis
Rheumatoid arthritis, which is so destructive to the small joints of the hands and feet, also affects the cervical spine (Fig. 26.4). The atlantoaxial joint is especially at risk because of the complex synovial folds around the transverse ligament of the atlas. If this ligament stretches, the atlas and head can slip forwards and the odontoid process presses against the cervical cord, producing quadriparesis.
 |
| Fig. 26.4 Rheumatoid arthritis of the spine with forward displacement at several levels. |
This is especially important to anaesthetists. The mouth will not open easily if the temporomandibular joint is affected. If the neck is also stiff, endotracheal intubation is difficult and the manipulation of the neck needed to intubate the patient is hazardous. Accordingly, patients with rheumatoid arthritis must always have the cervical spine examined radiologically before undergoing anaesthesia. All staff, particularly those in the recovery room, should be aware of the potential hazards of flexing a rheumatoid neck.
Treatment
A supporting collar is usually sufficient but atlantoaxial fusion may be needed if there is a neurological deficit or unremitting pain.
Acute torticollis
Severe and acute neck pain can be due to many things, including acute disc prolapse, muscle spasm, injury to an osteoarthritic facet joint, inflamed lymph nodes or an undiagnosed cervical dislocation.
Treatment
Treatment depends upon the cause. Most acute stiff necks settle with a collar, warmth and analgesia but serious injuries must be excluded first.
Cervical rib
A vestigial ‘rib’ of bone or fibrous tissue can run from C7 to the first true rib. When such a rib is present the lowest part of the brachial plexus runs across it and neurological symptoms in the arm may result. Pain down the inner side of the arm in the T1 distribution should raise suspicions of a cervical rib.
Treatment
Excision may be necessary if radiographs demonstrate a complete or incomplete cervical rib; conservative treatment with physiotherapy to improve the power of the shoulder girdle muscles has been ineffective. The operation is straightforward but the root of the neck is ‘tiger country’ and the operation must only be done by a surgeon who is very familiar with this area.
Congenital short neck (Klippel–Feil syndrome)
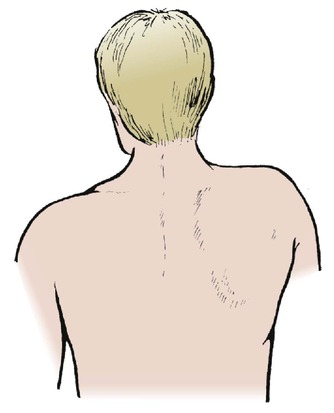
Klippel–Feil syndrome consists of a very short neck with fusion of two or more cervical vertebrae and restricted cervical movement (Fig. 26.5). The condition may be familial and is sometimes associated with scoliosis. Richard III (‘Deform’d, unfinish’d, sent before my time into this breathing world, scarce half made up’) may have had Klippel–Feil syndrome.
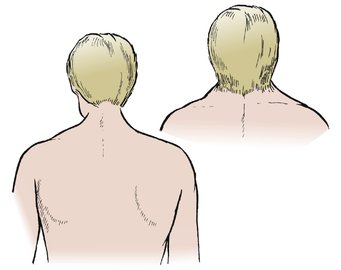 |
| Fig. 26.5 Klippel–Feil syndrome. A short webbed neck with low hairline. |
Treatment
No specific treatment is required but the scoliosis may need correcting.
Congenital high scapula (Sprengel’s shoulder)
Sprengel’s shoulder is a congenital deformity in which the scapula is small and abnormally high (Fig. 26.6). The condition may be bilateral. No cause is known except that there is a failure of development of the shoulder and the muscles attached to it and it is often associated with congenital spinal anomalies.
 |
| Fig. 26.6 Sprengel’s shoulder. A high fixed scapula. |
Treatment
Some improvement in position follows release of the muscles along its upper border if carried out at an early age.
Congenital hemivertebra
Congenital hemivertebra (Fig. 26.7) and other anomalies also occur and may be associated with neurological abnormalities.
 |
| Fig. 26.7 Congenital hemivertebra. There is an extra vertebra and rib on the right side. |
Neuralgic amyotrophy
Neuralgic amyotrophy is an odd condition which is probably due to a patchy demyelination of the brachial plexus. The symptoms may follow vaccination. Like meralgia paraesthetica, this condition is important because it has neurological features that may be confused with a spinal disorder.
Characteristic features are:
1. Sudden severe pain down the arm, similar to that of a disc protrusion.
2. Paralysis of parts of the shoulder girdle as the pain eases. The nerve to serratus anterior is said to be involved most frequently, producing a true winged scapula.
3. Muscle wasting is seen in the affected area.
Treatment
The pain usually resolves without treatment over a period of weeks, but the weakness may take up to 2 years to recover. Apart from reassurance and excluding other disorders, no treatment is required.
Acute stiff neck
Not all pain in the neck is due to a disc protrusion or cervical spondylosis. An acute stiff neck, perhaps due to a small muscle tear or a derangement of the facet joints, can occur for no apparent reason.
Treatment
The symptoms usually resolve spontaneously over a period of days or weeks. A supporting collar eases the pain and manipulation is sometimes helpful.
Lumbar spine
Back pain
In any one year, more working hours are lost from back pain than from any other medical condition. Back problems therefore take up much of the medical profession’s time. As many as 25% of referrals to some orthopaedic clinics are for back pain.
It is a bad principle to operate on a painful back unless a definite mechanical cause has been identified. In the past, painful backs were operated upon far too often and the results were poor. Many patients were no better and some were made worse by operation. Spinal surgery, particularly spinal fusion, earned a bad name, richly deserved because operation was often followed by severe pain and stiffness which disabled the patient more than the original condition.
Back pain alone is not an orthopaedic problem. It is best managed conservatively by departments of physical medicine and rheumatology, and to refer every patient with back pain to an orthopaedic surgeon is a little like referring every patient with headache to a dentist. Unfortunately, patients with backache are frequently referred to orthopaedic clinics for historical reasons.
Spinal surgery, however, is definitely an orthopaedic problem and many surgeons with a specialist interest in the spine also treat the painful spine. The spine should only undergo operation for anatomical lesions proven beyond doubt, which limits the common indications to the following conditions:
Indications for spinal operations
Indications for spinal operations
• Disc excision for proven disc protrusions with neurological signs.
• Instability caused by spondylolisthesis or unstable discs.
• Scoliosis, kyphosis and other spinal deformities.
• Some tumours and infections.
Acute back strain
Acute pain in the back radiating down to the knee but not beyond and without neurological abnormality is usually due to an acute muscle or ligament strain in the lumbar spine. The symptoms can be precipitated by a sudden violent movement or by a comparatively trivial movement following a period of hard work when the muscles are stiff.
Tall slim people with willowy backs and weak muscles are said to be especially prone to acute back strains, as are those in sedentary occupations, such as medicine, who live a life of ease during the week and punish themselves at the weekend with excessive gardening.
Those who sit for a long time and then have to lift heavy weights without an adequate ‘warm-up’, e.g. carriers who may drive for more than an hour with the spine flexed in a bumpy vehicle and then leap out of their seat to lift a heavy weight from the back of the van, are also very vulnerable.
The sacroiliac joints are also said to be subject to acute strains, but without conclusive proof. The joints have a large surface area, they have poor mechanical cohesion and violent twisting strains can cause severe pain around them.
Prevention
The ‘strain’ is usually the result of incorrect lifting and most can be avoided. Workers who have to lift heavy weights, including nurses who lift patients, should be taught correct lifting techniques (Fig. 26.8). Four principles are important:
 |
| Fig. 26.8 Incorrect and correct lifting. Keep the weight close to the body and the back straight. Lift with the knees. |
Correct lifting technique
1. Do not lift with the spine flexed; in this position, the weight is hanging on taut ligaments and stretched muscles, which makes them vulnerable to additional load. Instead, lift with the lumbar spine extended.
2. Keep the weight to be lifted as near to the body as possible. The further the weight is from the body, the more effort that has to be expended in lifting it.
3. Lift with the knees, not the back muscles.
4. Make the job as easy as possible. Ensure that there is good access to the load, if possible split it into lighter loads but, if it cannot be split, share the job with two or more people.
In the workplace, lifting can be made easier by storing goods at waist height and avoiding the need for a twisting motion while lifting or carrying or by using lifting equipment and conveyor belts.
Treatment
The following measures form the standard treatment for acute back injuries and are reliable; rest, analgesics and gradual mobilization are the most important:
1. Rest.
2. Analgesics.
3. Heat.
4. Gradual mobilization.
5. Lumbosacral brace.
6. Manipulation.
Rest. The patient should rest in the most comfortable position possible, which is usually on the back or side with the knees flexed. If lying in bed is painful it is perfectly acceptable to rest in a comfortable chair.
Analgesics. Any analgesic or NSAID can be used. Narcotics such as pethidine should not be needed.
Heat, either from a hot water bottle or a heat pad, is very comforting for pains arising from muscles and ligaments and the diagnosis should be reconsidered if heat does not help. The mechanism of relief is obscure, but is probably nothing more than old-fashioned counterirritation. Even if unscientific, patients find warmth helpful.
Gradual mobilization. As the pain subsides, gradual mobilization can be started, but the patient must be prevented from lifting weights and risking further injury for at least 6 weeks. This may be difficult if the patient is a hardworking self-employed worker who needs to get back to work to earn a living. It is nevertheless essential if recurrent strains are to be avoided.
Mobilization of the spine is important. If a full range of spinal movement can be achieved, it is likely that the muscle or ligament has healed and the presence of a full range of movement ensures that loads can be borne equally throughout the spine.
If movement is limited, further injury is probable. The stiff areas of the spine are more likely to be injured by sudden stress and the mobile areas will be taking more strain than normal. A good range of movement should therefore be achieved before the patient returns to work, and the range of movement maintained by an exercise routine.
Lumbosacral brace. If the patient insists on returning to work before full movement has returned, a lumbosacral support will lessen the risk of recurrence. A brace will support the back when the patient is lifting and, perhaps more important, will ‘remind’ patients of their condition so that they lift correctly.
Spinal supports should be worn only for pain relief or to protect the back when it is at greatest risk. If they are worn permanently the spine will become stiff, the muscles will take less strain, and further injury becomes more likely.
Manipulation. Manipulating an acutely painful back is occasionally harmful if there is some underlying undiagnosed pathology but is sometimes dramatically successful, particularly if the sacroiliac joint is affected. Manipulation is a skill which takes much training and should not be attempted by the inexperienced. Both osteopaths and chiropractors are skilled manipulators.
Differential diagnosis
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


