Chapter 43 Diagnosis and Treatment of Complex Regional Pain Syndrome
INTRODUCTION
Complex regional pain syndrome (CRPS) is the current terminology that refers to a disease first described during the era of the U.S. Civil War.46 Nomenclature relating to CRPS has varied over the years and included different descriptions, diagnostic studies, and treatments, few of which have been well studied. Adding to the confusion, this disorder has a variable presentation and there is no single test to confirm the diagnosis.7,34,50 CRPS is a clinical diagnosis of exclusion. It is difficult to interpret or gain useful information from the medical literature regarding this disease owing to the vague and varied nature of complaints and the 20 different terms that have been used to denote this syndrome.
CRPS is a chronic pain syndrome that usually follows tissue injury in which the patient experiences severe nondermatomal pain associated with painful responses to nonpainful stimuli, along with changes to the autonomic and trophic systems. The pain is associated with changes in skin color, temperature, sweating, edema, and range of motion. The pain is distinct in that it is out of proportion to the inciting event. This is problematic, because it often causes a delay in diagnosis as physicians believe the patient either is seeking recreational drugs or has a psychological disturbance or some other secondary gain issues.28
By definition, the previously named disease reflex sympathetic dystrophy (RSD) is now referred to as CRPS type I, and the formerly named causalgias are incorporated into the definition of CRPS type II. The International Association for the Study of Pain established the initial definition of CRPS to help eliminate confusion. This definition was later subdivided by Merskey and Bogduk into types I and II.45 The pain generator is described as being either sympathetically maintained pain (SMP) or sympathetically independent pain (SIP), depending on whether or not the sympathetic nervous system is involved.70
CRPS type I is defined as having
TABLE 43-1 Diagnostic Criteria of the International Association for the Study of Pain for Complex Regional Pain Syndrome Type I and Type II
CRPS, complex regional pain syndrome.
Reprinted with permission from Stanton-Hicks, M., Janig, W., Hassenbuch, S., et al.: Reflex sympathetic dystrophy: changing concepts and taxonomy. Pain 63:127–133, 1995.
CRPS type II has the same definition as type I with the exception that it is due to injury to a single peripheral nerve. In this respect, the region of disproportionate pain is initially within a dermatome (unlike CRPS type I that follows no dermatomal pattern).45 As the disease progresses, it can spread beyond a single dermatome.
Both CRPS types I and II have components of SMP and SIP.70 In fact, both SMP and SIP will frequently exist in each patient to varying degrees (Fig. 43-1). As is described later, there are periods when the nerve transmissions from the sympathetic nervous system will be interpreted by the body as pain. When this occurs, the normal signals to increase heart rate and blood pressure in response to fight-or-flight conditions not only affect the sympathetic nervous system but also cause pain. This source of pain is SMP. All other pain associated with CRPS is SIP. The only way to determine how much of the patient’s pain is due to SMP and how much is due to SIP is to perform a sympathetic nerve block. The pain relieved is SMP, and the remaining pain is SIP.68
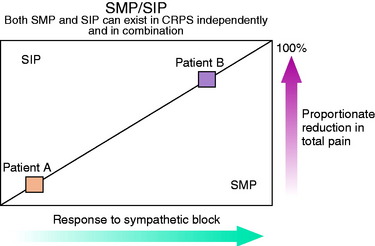
(Reprinted with permission from Janig, W.; Stanton-Hicks, M. [eds.]: Reflex Sympathetic Dystrophy: A Reappraisal Progress in Pain Research and Management, Vol. 6, Seattle, IASP Press, 1996, p. 83.)
Despite the complexity of the definition of CRPS, the hallmark of this disease is pain out of proportion to the inciting event. When this occurs, it is incumbent upon the clinician to be suspicious of CRPS and initiate treatment as soon as possible. Early management yields a more favorable outcome when initiated before the changes of skin color, temperature, and sweating occur.29
ANATOMY
To understand the basis of the pathology of CRPS, the clinician must have a rudimentary understanding of the human nervous system anatomy and function. At the clinical level, a more detailed understanding is not required. The intent is to describe the pathology in a way that makes sense to the clinician and so that it can be explained to patients in a manner that allows them to understand the disease and become active participants in their recovery. It is important to know that of the six predominant pathologic mechanisms that have been proposed to explain CRPS, none completely explains the clinical findings and results of treatment and all have shortcomings explained by other theories.3,7,50
CNS, central nervous system (brain and spinal cord); PNS, peripheral nervous system.
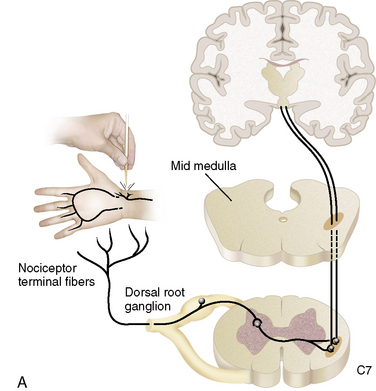
The nervous system consists of somatic and autonomic branches. The somatic system includes the central nervous system (CNS; brain and spinal cord) and the peripheral nervous system (PNS). The dorsal root ganglion is located in the paravertebral region, which contains the sensory nerve cell bodies.21 It is through the dorsal root ganglion that specialized ganglia transmit signals representing pain, pressure, and temperature from sensory nerves to the spinal cord.66
The autonomic nervous system is composed of sympathetic and parasympathetic divisions. Of importance is the sympathetic nervous system, which has cell bodies in the thoracolumbar paravertebral chain ganglions adjacent to the vertebral column. In the cervical region, the most inferior of the paravertebral ganglions is the stellate ganglion, which is believed to supply the majority of the sympathetic innervation to the upper extremities. In the lower extremities, the sympathetic innervation is carried through lumbar paravertebral ganglions.21
The sympathetic nervous system is responsible for the fight-or-flight response. This reaction is mediated by the catecholamine neurotransmitters, epinephrine and norepinephrine. These catecholamines stimulate receptors called α and β receptors. When α receptors are stimulated, the body responds with elevated heart rate and blood pressure, piloerection, and skin vasoconstriction. The β receptors stimulate increased heart rate, muscle vasodilation, and bronchial dilatation.40
In some cases, knee surgery as benign as arthroscopy can injure nerve structures and promote a CRPS type II. In the largest known study of 395,566 arthroscopic procedures, 234 nerve injuries were identified from operative notes.60 In a knee-specific study of 118,590 arthroscopies conducted by the Arthroscopy Association of North America, 63 neurologic complications were noted.60 In the same study, RSD was diagnosed in 44 patients. Both of these studies had a prevalence rate of nerve injury of less than 0.1%.
O’Brien and coworkers49 described 60 patients referred for RSD of the knee. Of these, 40 had developed symptoms after knee surgery (24 arthroscopic and 12 arthroplasty procedures). In the authors’ experience, many cases of CRPS begin with symptoms of saphenous neuritis. On the medial side of the knee, the saphenous nerve lies deep to the sartorius muscle. The infrapatellar branch of the saphenous nerve lies inferior to the medial joint line (see Fig. 1-23A). Formation of a neuroma may result from direct injury by the scalpel during anteromedial portal placement. Techniques for avoiding injury to the saphenous nerve and its infrapatellar branch include careful dissection through a 1-cm incision with identification of the nerve, transillumination with use of the arthroscope, and use of a 2-cm posteromedial incision with posterior retraction to deflect the needles anteriorly during inside-out medial meniscal repair.60
PATHOPHYSIOLOGY
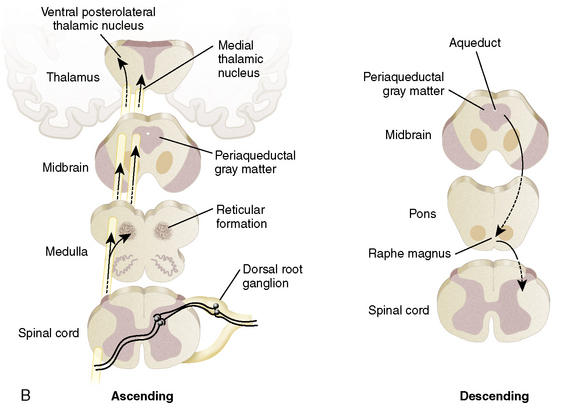
Six major theories have been devised to explain the findings and response to treatment of CRPS. Unfortunately, no single unifying theory is available. For that reason, only a few of the current theories are presented in this chapter (Fig. 43-2).
One hypothesis is that a pathologic interaction occurs between the somatic nervous system (in part responsible for sensations) and the autonomic nervous system (responsible for the fight-or-flight mechanism). Normally, these two systems do not directly interact. However, when a pathologic interaction does takes place, it occurs at a newly created abnormal synapse called an ephapse.3 An ephapse may take place in either the PNS or the CNS. The ephapse causes a type of short circuit to occur between the somatic and the autonomic nervous systems. The signals being sent from the CNS to the PNS to control heart rate and other factors are short-circuited to sensory fibers and are misinterpreted as pain signals being sent from the PNS to the CNS.27 The sympathetic nervous system drives the pain and, as a result, increased anxiety (which would normally increase blood pressure and heart rate) amplifies pain.
Another theory focuses on CRPS type II in which a specific nerve has been transected. An explanation for the CRPS findings from such a transection stem from the neuroma that forms as a result of the injury. Within this neuroma, the transected sensory nerve endings develop a catecholamine sensitivity through the up-regulation of α receptors (which respond to epinephrine from the autonomic nervous system).56 In this manner, when the sympathetic nervous system sends signals to increase heart rate, the increased density of α receptors in the sensory nerve endings of the neuroma are stimulated and transmit the pathologic pain signal back to the CNS.3 There is also a theory in which a similar up-regulation of α receptors occurs in the dorsal root ganglion.
Critical Points PATHOPHYSIOLOGY
Theories of the Mechanism of CRPS
The clinical findings of light touch hypersensitivity (allodynia) and cold hypersensitivity (hyperalgesia) are believed to occur through a central sensitization model termed the Raja model.55 In this model, pain receptors (nociceptors) up-regulate their α receptors. Because the body is constantly sending sympathetic signals, these nociceptors are being constantly stimulated, which reduces the CNS threshold for perceiving pain.58 Once again, changes occur in the dorsal root ganglion.22 The mechanoreceptors responsible for light touch sensation and thermoreceptors responsible for cold sensation instead produce an abnormal painful response when they stimulate the sensitized central pain neurons.
In the Raja model, treatment by sympathetic blockade is effective through the production of a temporary inhibition of norepinephrine release. By temporarily blocking the release of catecholamines, the sympathetic block relieves pain. By allowing the CNS to experience relief from pain, the central pain neurons may be desensitized (down-regulation of α receptors), resulting in a long-term improvement in the painful response to light touch.3
The change in regulation of α receptors also explains the change in appearance of the limb over time. Initially, an increase in α receptors causes excess stimulation that presents as a red, warm, and swollen limb (increased sympathetic function). Later, as the body adjusts and down-regulates the expression of α receptors, the same limb will take on a blue, cool, and contracted appearance.3 This can be explained to the patient with the following analogy. The patient controls the home computer (the CNS) and his or her children control the computer speakers (the PNS). If music is playing from the computer and the children like the song, they will turn up the volume to a painful level for the patient (perceived as pain by the CNS). In response to the pain of this loud noise, the patient (CNS) turns down the volume at the computer terminal, thereby decreasing the sound to a reasonable level (and decreasing the pain signal in the body). Unfortunately, by decreasing the strength of the signal from the computer to the speakers, other signals are also being transmitted weaker than normal. So, while the pain is decreased in the body, so is the strength of the sympathetic signal sent to the extremity, changing it from abnormally warm, red, and swollen to abnormally cool, blue, and constricted.
DIAGNOSIS
Clinical Presentation
The clinical presentation of CRPS is variable and comes in different stages with diverse appearances.54 The disease has no predilection for gender, age, or dominant extremity. The common cause is an initiating trauma to an extremity, which can be as obvious as a fracture or as minor as an ankle sprain. It can also occur in response to surgery, arthritis, and inflammatory conditions or reactions.7 In as many as 10% of cases, no initiating trauma can be identified.20
Sensory Disturbances
The hallmark finding of CRPS is pain disproportionate to the inciting event. The disproportionate response includes pain more intense than expected, lasting longer than expected, and expanding beyond the dermatomal region of the extremity. Pain is the body’s response to impending or ongoing cell death. With CRPS, the pain may be generated in the absence of cellular insult.36 Within hours to days after the initial noxious event, the pain becomes diffuse and expands beyond the site of the injury. As the condition progresses, the pain expands beyond dermatomal distributions in a stocking or glove pattern with a preference for distal limb involvement. Patients describe the pain as “burning and shooting” or as “deep, constant, and aching.” A classic finding is allodynia, pain with light touch. This is manifested during the physical examination and described by the patients during the history as the inability to tolerate pressure from bed sheets at night, clothing, and even air currents. The pain may fluctuate in intensity in response to many influencing factors. Aggressive physical therapy that is painful to the patient may worsen the condition. As the weather changes and becomes colder, the condition may worsen. Also, owing to the sympathetic nature of the disease, as patients become excited, their pain may worsen.
Sympathetic Dysfunction
Sympathetic dysfunction is manifested through changes in skin color, swelling, temperature changes, and cold intolerance. Classically, the limb will initially appear red, warm, and dry and progress over time to a mottled, bluish, cool, and moist condition. Note that the sudomotor function is opposite of what is normally expected. A red and swollen limb will normally be moist, and a bluish and cool limb will normally be dry. Side-to-side temperature differences can average 3.5° C in 80% of CPRS patients.77
Patients frequently report swelling that is extra-articular and painful. It is a prominent finding early in the course of the disease that decreases over time. Initially, the skin is edematous but gradually is replaced by skin that is tight, shiny, and lacking in normal skin creases.15
Of particular interest is a corresponding intolerance to cold. This finding is particularly sensitive for diagnosing SMP. Cold intolerance is often first encountered in physical therapy when cryotherapy is used to control swelling and produces a significant painful response.40 In the office, the clinician can use an ice cube test (Fig. 43-3) by applying ice to the sensitive region and asking the patient about the evoked sensations. The abnormal response the clinician seeks is a description of intolerable, burning pain. In the very early phase, the patient may describe the sensation evoked from the ice cube test as decreased cold sensation when compared with the contralateral limb. In a similar manner, cold weather can precipitate a painful flare.40


The natural history of sympathetic dysfunction falls into three stages. These stages do not follow a specific timeline and the patient can go forward and backward through the stages over time or in response to treatment. For this reason, the staging system has little clinical usefulness other than to understand the classic progression of the disease. The patient with CRPS may present with some or all of these symptoms, but may also present only with the symptom of disproportionate pain. The stages are acute, dystrophic, and atrophic.71
The acute stage usually lasts less than 6 months. During this time, the sympathetic system is hyperactive, yielding a limb with red, warm, and dry skin. The dystrophic stage begins after 3 to 9 months when the hyperactive sympathetic system finally diminishes to a period of decreased sympathetic activity. In this stage, the limb is cyanotic or mottled, cool, and moist, with thickening of the nails and coarse hair (owing to decreased blood flow to the skin). When the dystrophic stage persists long enough to produce an overall level of atrophy in the limb, the patient enters the atrophic stage. This stage is characterized by thin, tight, shiny skin, osteoporosis from prolonged decreased weight-bearing, and joint contractures from prolonged decreased range of motion.71
Motor Abnormalities
Motor impairment is a more recently appreciated symptom of CRPS.64 The deficits range from weakness to increased tone and hyperfunction. Even when motor abnormalities are grossly evident, electromyography tests remain normal. This finding suggests that the motor response of CRPS is centrally mediated, most likely at the spinal cord level.77 Initially, weakness can be attributed to disuse and expected muscle atrophy. Some patients develop pseudoparalysis that may extend to limb neglect. When hyperfunction is present, it manifests as action tremors, myoclonus, hyperreflexia, muscle spasm, and voluntary guarding.64 In longstanding illness, dystonia, apraxia, and lack of coordination may be present.77 In 50% of CRPS cases, patients show decreased range of motion, physiologic tremor, and weakness. About 10% of chronic cases will reveal dystonia in the hand or foot of the affected extremity.2
Psychological Issues
The clinician may respond to patients with CRPS and their disproportionate pain by believing they are malingerers or have fictitious disorders or other psychiatric overtones. However, as with many patients with a chronic pain syndrome, comorbid psychiatric disease either develops or promotes the pain syndrome.7,51 It is uncertain whether this is a cause or an effect of the CRPS, but in daily diaries kept by chronic pain patients, investigators found that yesterday’s depressed mood contributed to today’s increased pain, and yesterday’s pain also contributed to today’s depression, anxiety, and anger.20
It has been suggested by some authors that a particular personality type increases the risk for developing CRPS.18 However, this has never been proved.10 It is more likely that the emotional and behavioral disturbances are the result of chronic pain and loss of function. These psychological disturbances have been proved to resolve when the pain resolves.42,47
Objective Tests
Paravertebral Sympathetic Ganglion Blockade
Paravertebral sympathetic ganglion blockade is the best tool for diagnosing SMP-related CRPS and initiating treatment of CRPS. The patient is injected with a local anesthetic under fluoroscopic control. The local anesthetic is injected near the lumbar paravertebral sympathetic ganglion (for lower extremity disease) or the stellate ganglion (for upper extremity disease).40,70,77 Successful block of the ganglion is monitored by documenting vasomotor and sudomotor changes in the extremity. In a technically adequate block, the skin temperature of the extremity will approach core body temperature. In addition, in a stellate ganglion block, Horner’s syndrome (ptosis, miosis, and anhidrosis) will be induced. Relief of pain is due to blocking the SMP portion of CRPS. However, a placebo response as high as 33% has been documented and clinicians should be cautioned not to rely solely on this test for diagnosis.51
Related posts:
 Allografts: Graft Sterilization and Tissue Banking Safety Issues
Valgus Malalignment: Diagnosis, Osteotomy Techniques, and Clinical Outcomes
The International Knee Documentations Committee Rating System
Knee Ligament Function and Failure
Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes
Allografts: Graft Sterilization and Tissue Banking Safety Issues
Valgus Malalignment: Diagnosis, Osteotomy Techniques, and Clinical Outcomes
The International Knee Documentations Committee Rating System
Knee Ligament Function and Failure
Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


