Dental Injuries
Nathan P. Falk
Elizabeth M. O’Connor
INTRODUCTION
There are many benefits to participating in athletic activities, such as enhanced physical fitness and the enjoyment from competition. Sport, however, also increases the risk of sustaining an injury, especially injuries to the teeth and mouth.
Sports medicine physicians are in an ideal position to facilitate early intervention to preserve dental health and promote proper preventative strategies.
EPIDEMIOLOGY
An oral injury can be defined as dental avulsions; dental fractures; dental luxations; lacerations or contusions to the gum, cheeks, tongue, and lips; and jaw injuries (fracture, locked open or closed, temporomandibular joint (TMJ) pain, and chewing difficulty). A concussion from a blow under the chin can also be included (9).
Contact sports, such as basketball, hockey, and football, have a great risk of orofacial-related injuries. These injuries are the result of an increased risk of body-to-body or object/surface-to-oral cavity contact and are incrementally compounded by the speed of the sport. According to a study by Tesini and Soporowski (15), based on 159 injuries reported by pediatric dentists during a 1-year period, the sports receiving the most orofacial injuries were baseball and biking, followed by hockey and basketball.
Noncontact sports, such as golf, billiards, and bowling, have a much lower incidence of orofacial injury. Although not a contact sport, biking, as previously noted, has a great risk of orofacial injury (15).
Dental trauma data report that 25% of people ages 6-50 have sustained an injury to their anterior teeth (12).
The literature suggests that more boys than girls (3:1) are involved in orofacial sports-related injuries. Parents additionally seem more inclined to have their sons wear mouthguards as opposed to their daughters (15).
Studies have also shown that by the time a student graduates from secondary school, one out of three boys and one out of four girls will have suffered from a traumatic dental injury (15).
Injury rates appear to be highest from about 7 to 14 years of age (6).
ANATOMY
The tooth is composed of three layers: enamel, dentin, and the pulp chamber (Fig. 32.1).
The enamel is the most external layer of the three. Enamel protects the crown of the tooth because of its hardness and structure.
The next layer is called the dentin. The dentin is softer than the enamel and has dentinal tubules that contain neurovascular structures. When dentin is exposed, it is very prone to decay.
The internal structure of a tooth is the pulp. The pulp contains the blood vessels and nerves that supply the tooth from the jaw.
The periodontal ligament (PDL) connects the alveolar bone to the root and anchors the tooth in the socket.
FIELD-SIDE ASSESSMENT
Initial examination should be external, beginning with checking for lacerations of the head or injury to the neck. The TMJ can be externally palpated while the patient opens and closes the jaw. The opening pattern should be closely evaluated to check for deviation, which could indicate a unilateral mandibular fracture. Palpation of the zygomatic arch, angle, and lower border of the mandible should be checked for tenderness, swelling, and bruising to rule out bone fracture.
Intraoral examination of the lips, tongue, cheek, palate, and floor of the mouth should be done to check for laceration. Tenderness, swelling, and bruising of the facial and lingual gingiva need to be checked. The anterior border of the ramus can be palpated intraorally.
If there is a laceration to the lip or tongue, it must be palpated and, if need be, radiographed to rule out embedded foreign bodies.
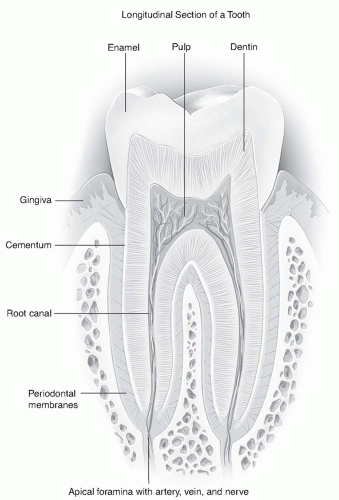 Figure 32.1: Anatomy of the tooth. |
SPECIFIC INJURIES
Trauma
Maxillomandibular relationships can increase risk for orofacial injury. Many studies have shown that the orthodontic status increases the rate of incisal trauma. A class 11 molar relationship (a malocclusion where the upper teeth protrude past the lower teeth, also called an overbite or buck teeth), having an overjet greater than 4 mm, having a short upper lip, having incompetent lips, and being a mouth breather will increase the chance of dental injury. A referral to an orthodontist to evaluate for orthodontic correction to reduce such risks is very important (14).
A tooth fracture can be classified as a root fracture, crown fracture, or a chipped tooth. The most serious complication of the tooth fracture would involve injury to the pulp. Pulpal involvement can be seen by examining the fractured area and looking for a bleeding spot or a red dot. This type of involvement can be painful, so care should be taken not to expose the tooth to air, saliva, and temperature changes. A patient with such a tooth fracture involving injury to the pulp should see their dentist for an examination and treatment on an emergent basis. A patient with dentin involvement should also not return to play and seek immediate dental attention. A patient with enamel-only involvement does not need immediate referral and can return to normal play with a protective mouthguard but must see a dentist for follow-up within 24 hours.
A tooth with a minor chip and without displacement does not need immediate dental attention but should be evaluated at a near future date, preferably within 24-48 hours (7). Any tooth fragments that can be saved should be given to the patient to bring to the dental examination.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



