Cycling
P. Gunnar Brolinson
Delmas J. Bolin
Bicycling for transportation and fitness has enjoyed a resurgence in the United States in recent years. Once considered a children’s toy, the bicycle is now a favorite fitness avenue for adults, from stationary spinning to mountain biking. With this surge in popularity has come an increase in the number of bike-related injuries, which account for over half a million emergency room visits annually (1). The actual number of injuries is certainly much higher, as many injured cyclists self-treat and never seek care. Of the approximately 800 riders who die each year, nearly two thirds are due to traumatic brain injury sustained by riders not wearing a protective helmet (1). Cycling’s physical demands place the rider at risk for a variety of traumatic and overuse injuries. An osteopathic approach to many of these overuse injuries can reduce time away from training and improve rider performance.
HISTORY
Cycling is an ancient sport with origins dating back to 2300 B.C. in China. The modern era of cycling began with de Sivrac’s Celerifere in France in the 1790s. This hobby-horse was a heavy, rigid, two-wheeled wooden machine with a central backbone. The rider propelled himself by paddling his or her feet on the ground. Initially used for gardening, these early bikes were later raced along the Champs Elysées. In perhaps the earliest example of cycling overuse injuries, young men frequently developed hernias from straining to steer the hobby-horse (2). In 1817, Baron Karl von Drais introduced the Draisienne, which had a steering bar connected to the front wheel. These rigid, solid-wheeled machines transmitted every bump in the road to the rider and were nicknamed bone-shakers.
In the 1830s, a Scottish blacksmith named MacMillan added foot pedals to the wheels. By the 1870s, the Penny Farthing or ordinary bicycle was introduced. The hallmark of this classic design was a very large front wheel with attached pedals paired with a small back wheel (3). The wheel ratio was the secret to the increased speed and efficiency of this bicycle; the larger the wheel, the greater the distance traveled with each revolution of the pedals. Almost as soon as the self-propelled bike was available, records began to be kept. In 1876, the first 1-hour cycling record (25.508 km) was recorded in England (4).
The Penny Farthing offered a tremendous mechanical advantage to earlier designs and made the bicycle an efficient mode of transportation but more difficult to ride than earlier designs. Riders were commonly injured when the front wheel of this model caught against the uneven stones or deep ruts in primitive roads. The sudden stop often propelled the rider head-first from a significant height onto his head, the origin of the phrase “taking a header” (3).
This problem was partially solved by the development of the safety bike, introduced first in the 1830s, which featured smaller, equal-sized wheels. During the late 1800s and early 1900s, improvements to the safety bike, including chain-drive systems, air tires, and gear-change technology, resulted in the modern bicycle. During this time bicycles were widely used for transportation. Bicycle racing became extremely popular and drew large crowds. Champion cyclists were celebrities and the highest paid athletes of the time (5).
TABLE 28.1. RELATIVE PERCENTAGE OF INJURIES TO MEN AND WOMEN PARTICIPATING IN A NATIONAL MOUNTAIN BIKE RACE | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The bicycle’s basic efficiency was a main factor in its rise to popularity. Walking consumes 0.75 calories per kilometer, whereas a bicycle increases the speed fourfold while decreasing caloric expenditure fivefold.
The development of the motorcar as affordable and faster transportation during the early twentieth century resulted in the bicycle becoming primarily a children’s toy. During the later part of the twentieth century and the beginning of the twenty-first century, cycling has enjoyed renewed interest due to physical, psychological, and ecological benefits. Cycling is now one of the largest participatory sports for recreational and competitive athletes.
EPIDEMIOLOGY
Injury patterns in biking are dependent upon numerous factors including the age and experience of the rider, terrain, time of day, speed, and the type of riding. Children are much more likely to be injured than adults, with the peak incidence of injury between the ages of 9 and 15 (6,7). Boys are two to three times more likely to be injured (7). Among adult riders, traumatic and overuse injuries are influenced by type of riding. Long-distance road biking predisposes the rider to unique overuse injuries including neuropathies of the hands, perineum, and feet. Mountain bikers are more prone to traumatic injury. These injuries peak in riders between 20 and 39 years of age and usually occur from loss of bike control on unfamiliar downhill terrain at excessive speed (8). Prospective injury data have recently been reported for a major U.S. mountain bike race. In this competitive setting, women had nearly twice the risk for injury as men and were four times more likely to sustain a fracture. Table 28.1 shows the relative percentages of injuries in competitive male and female mountain bikers (9). The distribution of injuries is relatively unaffected by gender.
BICYCLE DESIGN
There are generally five types of bicycle design: racing, sport/touring, mountain, hybrid, and juvenile/specialty bikes (tandem, stunt bikes, etc). The design dimensions of the different bike types are subtly influenced by their function. Likewise, the proper fit of a bike to the rider is highly dependent upon what the rider intends to do.
Figure 28.1 shows the frame and main components of the typical bicycle. A road bike has steeper frame angles (e.g., between seat stay and chain stay) that produce a more upright geometry (10). Road cyclists usually ride on a lightweight bike in an aerodynamically advantageous crouched position on narrow, low-resistance tires. Road bike components are selected for
performance and speed. In contrast, mountain biking typically involves off-road riding on dirt roads or narrow trails (single track). The mountain bike has a heavier frame, which lowers the center of gravity, and is equipped with wider, deeper-treaded tires than a road bike. Mountain bike frames have more shallow angles (10), allowing the rider to sit back placing more weight on the back wheel for traction while climbing. Advanced components, such as front and rear suspension, may be required on more advanced single-track rides with steep descents and jumps.
performance and speed. In contrast, mountain biking typically involves off-road riding on dirt roads or narrow trails (single track). The mountain bike has a heavier frame, which lowers the center of gravity, and is equipped with wider, deeper-treaded tires than a road bike. Mountain bike frames have more shallow angles (10), allowing the rider to sit back placing more weight on the back wheel for traction while climbing. Advanced components, such as front and rear suspension, may be required on more advanced single-track rides with steep descents and jumps.
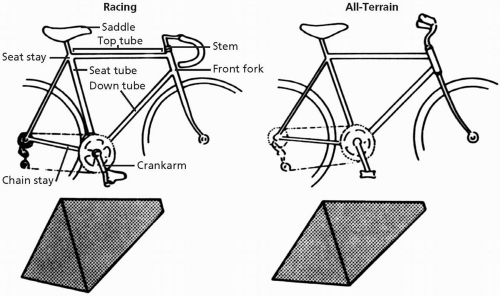 FIGURE 28.1. The dimensions of road and mountain bikes. The steeper angles of the road bike produce a more upright geometry. Main components are labeled. (Adapted from Burke E. Proper fit of the bicycle. Clin J Sport Med 1994;13:1-14.) |
Hybrid bikes are a combination of touring and mountain bikes. These bikes have the geometry of a road bike, but with a stronger frame and more heavily treaded tires. These characteristics permit their use on a variety of terrain, including paved, gravel, or dirt trails.
BICYCLE FIT AND PERFORMANCE
Proper bicycle fit not only prevents injury but also optimizes efficiency, whereas an improperly fitted bicycle predisposes the rider to injury. Every component of the bike from the saddle to the length of the crankshafts to the handlebar stem is important and should be customized for the rider to optimize performance.
The first step to ensuring proper fit of the bicycle is to determine the correct frame size. While straddling the bike, the top tube should be 1 to 2 inches (2.5 to 5 cm) below the crotch for road bikes, and 3 to 6 inches below the crotch for mountain bikes.
A number of different measurements for estimating seat height are available. The saddle should be even with the trochanter when the rider stands barefoot next to the bike (10). We have found that a rider can quickly estimate the correct position by sitting on a supported bike with the pedals in the 6 and 12 o’clock positions. When the seat is at the correct height, the leg should be nearly fully extended when the pedal is in the 6 o’clock position. At this height, power output is maximized and oxygen consumption and calorie expenditure are minimized (11,12). Seat height influences muscle recruitment, movement patterns, and joint forces during pedaling (13,14,15). Mountain bike saddle height is typically lower than that of a road bike, giving the rider a lower center
of gravity, greater maneuverability, and stability. Subsequent changes to saddle height should generally be in small (0.25 in.) increments spaced out over a few riding sessions (10). The saddle should be level, or tilted slightly downward to relieve pressure on the perineum during the ride.
of gravity, greater maneuverability, and stability. Subsequent changes to saddle height should generally be in small (0.25 in.) increments spaced out over a few riding sessions (10). The saddle should be level, or tilted slightly downward to relieve pressure on the perineum during the ride.
On a road bike, the saddle should move fore or aft so that when the pedal is in the 9 o’clock position, a plumb line can be dropped from the anterior patella through the middle of the pedal. In contrast, the mountain bike saddle should be positioned so that the knee is 2.5 to 15 in. (1 to 6 cm) behind the axle of the pedal in the 9 o’clock position. This allows for more relative weight to be placed on the rear wheel when climbing (10). The ball of the foot should be centered over the pedal axle.
The handlebars are positioned at least 2 in. (5 cm) below the saddle height. Taller riders typically place the handlebars lower, to achieve the most aerodynamic riding position. The stem length may be customized for comfort. The proper handlebar position and stem length can be estimated by placing the tip of the olecranon against the saddle front; the fingertips should rest on the horizontal center of the handlebar.
The crankarm length influences knee and ankle angles, revolutions per minute (rpm), and leverage. The standard crankarm (35 ft [170 cm]) fits most riders from 5 to 6 feet tall. A shorter crankarm is better for low-gear, low-rpm pedaling such as climbing. Longer crankarms are better for pushing higher gears on flat surfaces (10). Power output studies show optimal output when crankarm length is proportionate to lower extremity length (trochanter to foot) (16). Higher-performance cyclists require longer than expected crankarm lengths to optimize power output at their usual higher pedal rpm (17).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


