Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Vimala Ramachandran
Thomas F. Varecka
DEFINITION
Malunion of the radial or ulnar shaft can lead to pain, loss of motion, loss of strength, and instability at the level of the wrist or elbow.
Malrotation, angulation (with narrowing of the interosseous space between the radius and ulna), shortening, and loss of the radial bow have been shown in various studies to lead to decreased functional outcomes.4,5,9,10,12
Arthritis has been reported at the level of the proximal radioulnar joint (PRUJ) with long-standing malunions, although the distal radioulnar joint (DRUJ) is most commonly affected by forearm malunions.11
ANATOMY
The forearm can be thought of as a ring, connected at the PRUJ, the interosseous membrane, and the DRUJ (FIG 1).
Force transmission occurs through the interosseous membrane from the radius distally to the ulna proximally.
Radius
The radius lies parallel to the ulna in supination. With pronation, it rotates around the ulna while the ulna maintains its position throughout forearm rotation.

FIG 1 • Lateral projection of the radius and ulna. Relationship of the interosseous membrane to the radius and ulna during forearm rotation. The fibers of the interosseous membrane are longest with the forearm in neutral position and shorten in both pronation and supination.
The radius shaft is triangular in cross-section, with the apex toward the attachment of the interosseous membrane.
It contains three surfaces: anterior, lateral, and posterior.
The shaft possesses a gentle bow, with the volar surface concave and the dorsal and lateral surfaces convex.1
Ulna1
The ulna is a long bone that has a triangular cross-section in the proximal two-thirds and a circular cross-section distally.
It possesses three surfaces: anterior, posterior, and medial.
The proximal half of the shaft is slightly concave volarly. The distal half is relatively straight.
The PRUJ consists of the radial head, the radial notch, the annular ligament, and the quadrate ligament.
The DRUJ consists of the sigmoid notch, the ulnar head, the dorsal and volar radioulnar ligaments, the extensor carpi ulnaris (ECU) subsheath, and the triangular fibrocartilage complex (TFCC).
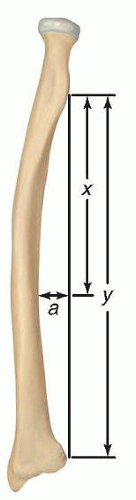 FIG 2 • Measurement of the location and magnitude of the radial bow. The distance y represents the length of the radius as measured from the bicipital tuberosity to the ulnar aspect of the radius. Line a, drawn perpendicular to y from the point of greatest curvature of the radius, represents the magnitude of the radial bow (expressed in millimeters). The distance x represents the length of the radius from the bicipital tuberosity to the point where a intersects y. The location of the radial bow is calculated by x/y × 100. (Adapted from Schemitsch EH, Richards RR. The effect of malunion on functional outcome after plate fixation of fractures of both bones of the forearm in adults. J Bone Joint Surg Am 1992;74(7):1068-1078.) |
PATHOGENESIS
Both-bone forearm fractures occur through a variety of mechanisms, including indirect trauma (such as falls on an outstretched arm or motor vehicle accidents) and direct trauma (such as blows to the forearm).
Acute fractures treated closed or with intramedullary nailing techniques are more likely to heal malunited.7,8
A torsional deformity of greater than 30 degrees in the radius leads to significant loss of forearm motion.4
Changes in the length-tension curve of the interosseous membrane may also account for loss of rotation.12
NATURAL HISTORY
Fifty degrees of supination and 50 degrees of pronation are needed for activities of daily living.6
Patients with untreated forearm malunions may experience loss of forearm rotation, PRUJ or DRUJ instability, wrist pain, loss of strength, and arthritis at the PRUJ.11 The severity of the symptoms depends on the degree of malunion and the corresponding alteration in degree and location of the bow of the radius.
Malunions of 10 degrees or less lead to less than a 20-degree loss of forearm rotation and hence are clinically insignificant.7
Patients with greater than 15 degrees of malalignment or loss of the radial bow will have clinically significant loss of motion and strength if left untreated.
PATIENT HISTORY AND PHYSICAL FINDINGS
The preoperative evaluation for patients with forearm malunions includes a detailed assessment of the patient’s functional limitations as well as documentation of elbow and wrist range of motion, the supination-pronation arc of the forearm, and the stability of the PRUJ and DRUJ.
Physical examination
The skin is inspected for scarring or previous incision sites.
Muscle bulk and tone are examined.
The wrist, elbow, and malunion site are palpated for tenderness.
Range of motion
The flexion-extension arc of the elbow is measured with the shoulder at 30 degrees of forward flexion.
Rotation of the forearm is ascertained with the humerus stabilized against the chest wall and the elbow at 90 degrees of flexion.
Wrist flexion and extension are determined with the forearm in neutral rotation.
Joint loss of motion may indicate location of pathology.
A high degree of motion loss will lead to functional deficits.
PRUJ and DRUJ
Stability of the PRUJ is assessed by palpation during passive pronation and supination.
The DRUJ is evaluated by stressing the ulna volarly and dorsally while stabilizing the radius.
Subluxation of the ulnar head or the ECU is evaluated during passive range of motion (ECU subluxation test).
The piano key test can also be used to assess for an unstable DRUJ. Patients with a positive piano key sign will have an ulnar head that shifts volarly with a minimal volarly directed force and then rebounds dorsally once that force is removed, much like a key in a piano.
Pain with compression of the radius and ulna at the level of the DRUJ may also be indicative of DRUJ instability or arthritis (DRUJ compression test).
Neurovascular examination
The examiner should check for anterior interosseous nerve (OK sign), posterior interosseous nerve (PIN) (thumb extension), and ulnar nerve (abduction-adduction of fingers) function.
Inability to perform tasks identifies nerve injury.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Anteroposterior (AP) and lateral radiographs of both forearms should be obtained (FIG 3A,B).
Both the bicipital tuberosity and the radial styloid should be visualized for the film to be adequate.Related posts:
 Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures
Fragment-Specific Fixation of Distal Radius Fractures
Vascularized Bone Grafting and Capitate Shortening Osteotomy for Treatment of Kienböck Disease
Operative Treatment of Metacarpal Fractures
Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures
Fragment-Specific Fixation of Distal Radius Fractures
Vascularized Bone Grafting and Capitate Shortening Osteotomy for Treatment of Kienböck Disease
Operative Treatment of Metacarpal Fractures

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


