Conditioning and Training Programs for Athletes/Nonathletes
Sally E. Nogle
Jeffrey S. Monroe
Section A General Principles
The information outlined in this chapter comes from scientific application of theories and principles of exercise physiology, using both animal and human studies. The chapter begins with the adult male competitor: the type of participant used most often in studies done on training and conditioning. A discussion of the young athlete, the female athlete, and the older athlete follows.
Metabolic Specificity
To maximize its beneficial effect, any training program must develop the specific physiological capabilities required to perform a given sport or activity (see Chapter 2). The most important physiological capability to be enhanced is the ability to supply energy (adenosine triphosphate [ATP] and the substrate phosphocreatine [PC]) to working muscles. ATP can be supplied in any of following three ways to the muscles:
ATP-PC system (anaerobic) used in maximum intensity exercises under ten seconds or less
Lactic Acid System (LA) (anaerobic) functions in high intensity exercise three minutes or less
Oxygen or aerobic system is utilized in activities greater than three minutes
As illustrated in Table 6A.1, the capacity and the rate at which energy (ATP) can be supplied by these three systems in the body differ. The rate of supply can be referred to as “power.” The predominant energy source will be a function of the total amount and rate of energy demanded by that exercise (see Table 6A.2). When a training/conditioning program is constructed, such a regimen logically should specifically increase the capacity of the energy system used most often in that particular sport.
Factors to consider for achieving maximal benefits from a training program include the following:
The mode of exercise used during training should be the mode used in the performance of the sports skill. For example—unless he is injured, an athlete should not train for running by swimming. However, training effects induced by running, although still specific, do appear to have beneficial cross-over effects for other sports.
Training effects tend to be specific to muscle groups. The major objective of physical training is to cause specific and efficient biological adaptation to improve performance in specific events. Therefore the muscle groups used for these events must be trained.
Four major principles should be applied to any training/conditioning program:
Specificity. Specific training elicits specific adaptations, enhancing specific actions.
Overload. Overload refers to exercising at above normal levels, and is achieved by manipulating combinations of training frequency, intensity, duration, and type of
activity. This is also known as the SAID Principle, specific adaptations to imposed demands.
TABLE 6A.1 Capacity and Power of Three Energy Systems in Untrained Male Subjects
Energy System
ATP Production
Capacity (Total mol)
Power (mol/min)
ATP-PC
0.6
3.6
LA
1.2
1.6
O2
∞
1.0
ATP % adenosine triphosphate; PC % phosphocreatine; LA % lactic acid; O2 % oxygen.
Source: Fox EL. Physical training: methods and effects. Orthop Clin North Am 1977; 8:533-548, (1).
Individual differences. People respond and perform differently to similar stimuli. Individual variations should be taken into account in the construction of any training program. A specific training program that works for one athlete may not for another.
Reversibility. This refers to the principle of detraining. Unfortunately, the beneficial conditioning effects of exercise training are transient and reversible, so conditioning should be continuous in nature. A swift and significant detraining effect may be seen when a person stops exercising. After only 2 weeks of inactivity, significant reductions in work capacity can be measured (2).
Necessary steps in the construction of a conditioning program should include the following:
Consider the predominant energy system used (see Table 6A.2 and Figure 6A.1).
Select an appropriate training regimen (see Table 6A.3).
Any training prescription and its content should include movement patterns specific to the sport and/or position to enhance motor unit recruitment patterns. Repetitive motor skill work will augment neuromuscular skills and enhance subsequent performance.
TABLE 6A.2 Performance Time and Energy Systems
Performance Time
Predominant Energy System(s)
30 sec
ATP-PC
30 sec-1 ½ min
ATP-PC and LA
1 ½-3 min
LA and O2
3 min
O2
ATP = adenosine triphosphate; PC = phosphocreatine; LA = lactic acid; O2 = oxygen.
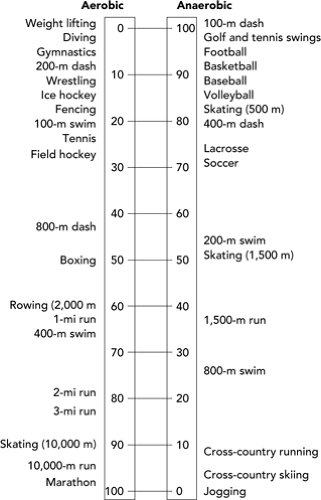
Figure 6A.1 A comparison of aerobic and anaerobic contributions of adenosine triphosphate (ATP) during the performance of various sports.
To prevent boredom and overuse injuries, introduce variability into the training program. Overuse injury is a significant result of lack of training variability.
Exercise Prescription
For an in-depth justification of the recommendations given here, please refer to the American College of Sports Medicine (ACSM) statement on quality and quantity of exercise (Appendix 5A). As mentioned earlier, the four major training components of conditioning are frequency, intensity, duration, and mode of activity.
Frequency
Training should occur three to five times per week. In a primary care setting, the practitioner must clearly ask a patient to set aside time for an exercise program. This time must be sufficient for the complete workout and it should have a high priority on the individual’s daily schedule.
TABLE 6A.3 Definitions of Various Training Methods and Development of The Energy Systems | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Intensity
Intensity is the factor that varies the most when individuals first begin an exercise program. Consider the following when making recommendations about intensity of exercise:
Determine either the maximum aerobic capacity (VO2max) or maximum heart rate (MHR) (beats/minute). MHR levels adjusted to age and fitness have been estimated using graded exercise testing (see Table 6A.4). Another convenient, reasonably accurate method is MHR = 220—the age of the patient.
An appropriate training level should be established within these ranges:
VO2max—Range—50% (beginners) to 85% (elite athletes).
MHR—Range—60% (beginners) to 90% (elite athletes); average—70%.
Fine adjustments need to be made considering the following:
Motivation.
Musculoskeletal limiting factors.
The body habitus—the more obese the individual is, the less intense and weight bearing a training program should be at the beginning.
Advise the patient to monitor pulse rate every 10 to 15 minutes through the course of activity. This can be done by educating the patient to take either carotid or radial pulse.
Duration
Fifteen to sixty minutes of continuous aerobic activity is recommended. The frequency of exercise is a factor with a wide and flexible range. An individual who exercises only three times a week needs a longer exercise period (usually 45–60 minutes) than someone who exercises five to six times a week, and who may only need 15 to 30 minutes of exercise. Consider the “F × I × D” product, frequency × intensity × duration, to get a rough idea of work done over a period. A desirable exercise program for the recreational noncompetitive adults will be of longer duration with low to moderate intensity because of better compliance and less chance of injury.
Mode of Activity
Improving aerobic capacity requires the use of large muscle groups, continuous exercise, rhythmic repetitive movement, and stimulation of the aerobic energy system. It should be mentioned that anaerobic exercise is usually static, very intense in nature, and only results in minimal beneficial effect on the cardiovascular system. Anaerobic exercise will increase muscular strength and endurance. This type of exercise is generally contraindicated for patients with heart disease and/or hypertension (see Table 6A.5). Consult Tables 6A.4 and 6A.5 for approximate sport-specific energy expenditures.
TABLE 6A.4 Age-Fitness Adjusted Predicted Maximum Heart Rate (MHR) for Three Levels of Fitness | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 6A.5 Diseases that Contraindicate Anaerobic Exercising for Recreational Athletes | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
Additional Concepts
The primary care physician should also take into account the following considerations in prescribing an exercise program. They are not part of the five major factors normally considered in an exercise program, but they represent important additional information.
Detraining. A total loss of conditioning following rest or inactivity takes place between 10 and 34 weeks after training ceases. Stopping may be voluntary (vacations, other obligations) or involuntary (illness, injury).
Epidemiological studies. It appears that more injuries occur in weight-bearing activities than in non–weight-bearing ones. In addition, the only consistent biological characteristic associated with noncompliance or dropout from an exercise program is obesity (4). For this reason, we suggest foregoing most weight-bearing exercise until later in the program, especially for those patients who are obese.
Energy equivalents. These rough equivalents can give the prescribing physician some idea of possible “cross-over” training activities that can be used in the event of injury. The approximate formula is: 9 units biking = 4 units running = 1 unit swimming. This formula is very useful for determining relative rest when treating overuse injuries.
Age should not be a deterrent to training. The major consideration of age is a need for a longer period of adaptation. Natural decreases in functional status that occur with age can be delayed or even reversed. Those decreases are outlined in Table 6A.6. The effect of a
chronic disease such as osteoarthritis may be reversed by the application of the right amount of exercise and movement for the affected joints.
TABLE 6A.6 Age-Related Decreases in Functional Status
Cardiovascular system
↓Maximum heart rate
10 beats/min/decade
↓Resting Stroke Volume
30% by 85 yr of age
↓Maximum Cardiac Output
20%-30% by 65 yr of age
↓Vessel compliance
↑Blood pressure 10-40 mm Hg
Respiratory system
↑Residual volume
30%-50% by 70 yr of age
↓Vital capacity
40%-50% by 70 yr of age
Nervous system
↓Nerve conduction
10%-15% by 60 yr of age
↓Proprioception and balance
35%-40% ↑ in falls by 60 years of age
Metabolism
↓Maximum O2 uptake
9%/decade
Musculoskeletal system
↑Bone loss: male >35 female >55
l%/yr
↓Muscle strength
20% by 65 yr of age
↓Flexibility
Degenerative disease or inactivity
Source: Compiled from data: Fitzgerald PL. Exercise for the elderly. Med Clin North Am 1985;69(1):189.
A program that occurs fewer than 3 days a week, is less than 50% VO2max levels in intensity, and has a duration of less than 10 minutes a day is inadequate to achieve a training effect.
Major Components of a Good Training Program
Preconditioning
Preconditioning is absolutely imperative at the beginning of exercise. Preconditioning gives the body time to adjust and provide a safer, more measured response to exercise. It is less taxing on the cardiovascular system and causes fewer injuries. Ten to 14 days at intensity levels lower than normal is advocated. For example, the use of the run-walk (run until tired, then walk, then run again) is appropriate as a preconditioning program for jogging. Another example is the use of low gear biking on level ground before adjusting to high gear cycling on hills.
Warm-Up
A warm-up lasting between 5 and 10 minutes should precede the beginning of every exercise program. The two components to any warm-up program are low intensity activity and stretching. The order is important. Warm-up should begin with 5 minutes of low intensity activity, preferably the same type that will be done during exercise, although jogging is a good all-purpose warm-up activity. The purpose of warm-up is to increase blood flow to major muscle groups, gradually increase the heart rate, reduce muscle stiffness, facilitate enzymatic activity, and ready the body for more strenuous effort. This should be followed by approximately 5 minutes of slow, gentle stretching (no bouncing) of major muscle groups, particularly those that will be heavily used during exercise. The warm-up period is not benign. Overstretching, “ballistic,” and/or improper stretching have caused many acute soft tissue injuries (please refer to Chapter 8 for figures on poor stretching techniques). The period can be expanded to include 5 to 10 minutes of muscular strength and endurance exercises (push-ups, pull-ups, sit-ups, etc.). It should be noted that the warm-up phase should never be eliminated.
Exercise Period
Discussed earlier in this chapter.
Cooldown
This is another transition period and should consist of low intensity activity such as jogging and some light stretching. This important component should last 3 to 5 minutes. It covers an extremely dangerous physiological time in the course of a workout session. Just as the warm-up physiologically prepares an individual for the exercise stimulus, the cooldown allows for proper recovery from exercise. During the cooldown, there are rapid changes in peripheral vascular resistance and venous return so that the induction of life-threatening cardiac arrhythmias is most likely to occur. This part of the training program allows the body (specifically the cardiovascular system) to accommodate and adjust to the non–exercise mode.
Progression—Part 2
If an increase is contemplated in an exercise program, it should be accomplished slowly over a period. There should be no pain or history of recent injury before an increase is undertaken.
Never increase two of the three components of a training program simultaneously; (frequency, intensity, and duration). Only one component at a time should ever be increased, and that too on a gradual basis. For example, a patient on a jogging program should be advised to add no more than 10% to 15% at a time to the distance or time being run, with the increases coming no more often than every 2 weeks while the same frequency and intensity are maintained.
Return from Injury
Relative rest versus absolute rest. Relative rest refers to decreasing the training regimen but allowing an athlete to train at a lower level. Absolute rest pulls an athlete completely off training. From a primary care perspective, we feel that patient compliance is easier to achieve and there is less muscle atrophy and detraining if the relative rest concept is advocated for most patients.
Alternative activity. There are many times in the treatment of injuries when a particular mode of activity is contraindicated. An alternative activity is an option for some patients. The basic premise is to decrease the force load placed upon the body by the activity in question (see Table 6A.7).
Light Intensity Training Program
The objective of Light Intensity Training (LIT) is to steer away from dogma concerning a return to activity after injury, and allow an individual some self-determination in how quickly the return is accomplished. This program can be instituted when the individual is able to ambulate or perform “activities of daily living” without symptoms (pain, swelling). A specific activity is begun on an every other day basis and at a very low level without regard for duration or intensity. The three options to be considered during and after this trial return to activity are as follows:
If pain and/or swelling develops during the activity—stop all activity immediately and decrease the following day’s activity by 25% (at the start, less as distance or duration of activity increases).
If pain and/or swelling develop after exercise is completed—continue the following day at the same level, but do not increase the level of activity.
TABLE 6A.7 Equivalent Force Loads
Jumping
10-14× body weight
Running
4-7× body weight
Walking
1× body weight
Biking
0.25-0.50× body weight
Swimming
0× body weight
If pain and/or swelling are not present during or after activity—increase activity slightly (up to 25% at the start, less later).
This program allows an orderly stepwise return to a previous training regimen and incorporates the cooperation and help of the patient.
Section B The Young Athlete
This section presents those aspects of conditioning/training programs for young athletes that might differ from what already has been discussed.
It is appropriate to discuss the role of exercise in adolescents and younger children. The leadership of a knowledgeable primary care physician who can lend assistance to a community organizing a youth sports program can be powerful and invaluable. It may well represent one of the most effective preventive medicine interventions a physician can undertake in his community. Childhood and adolescence are the most active periods of life, and interest in exercise and sports is at its peak. Unfortunately, medical science has yet to quantify, or even describe with any degree of accuracy, the major characteristics of growth and exercise and how they relate to each other. The effect of both long- and short-term exercise on physical training of youth remains a matter of speculation. It should come as no surprise that medical science has difficulty setting fitness guidelines for preadolescents and adolescents. Nevertheless, a summary of exercise prescription for the youth is useful even if difficult to execute.
The Prepubescent Athlete
Unique physiological characteristics of the young athlete include the following:
Physical growth. Of the three growth spurts occurring in humans, the first (inuteral) is nutritionally and genetically determined, and the second (occurring at approximately 54–60 months of age) takes place before major athletic involvement begins. However, the third (rapid growth associated with puberty) is affected by the amount of exercise.
Exploration of new areas of interest. Inquisitive youngsters often look upon sports activity as a new experience.
Maturation. With the initiation of maturational changes during puberty, there is an augmentation of strength, endurance, and neuromuscular skills.
Body proportion changes. During the adolescent growth spurt, approximately 15% of the adult height and 40% of the skeletal mass are achieved.
Body composition alterations. Prepubertal boys and girls have approximately the same percent body fat, but
during pubertal growth male body fat decreases whereas female body fat increases. In addition, muscular body strength in the male increases more than in the female.
Other considerations. In addition to the physical changes, massive psychological and sociological changes occur simultaneously, affecting to a great extent the developing child and his/her attitude to athletic activities.
A summary of pertinent questions that might be asked of a physician about prepubescent training regimens include the following:
Is such training dangerous to the preadolescent epiphysis? No. In a large study of athletes with epiphyseal injuries, 98% resulted in uneventful recovery with no major medical intervention needed once proper diagnosis was made (5).
Are there any special nutritional or thermoregulatory considerations for children in training? No. The nutritional requirements of this group vary little from those of nonathletes of the same age group. Heavy growth demands dictate the rate of nutritional uptake. Little in the way of special diet or supplements is needed for young athletes as long as they eat a normal, well-balanced diet (6,7). The only special consideration would be replacing those calories used in training with pure complex carbohydrates. The thermoregulatory mechanism of the young athlete is extremely efficient, although the amount of sweating is less than in an adult. The capacity to thermoregulate remains higher and more efficient in the prepubescent child (8).
Do growth and development benefit from training or are they impeded by exercise? There appears to be no data to accurately answer this question, but several studies have indicated that a “normal” amount of exercise is beneficial for growth and development. Excesses in exercise can have a harmful dampening effect on growth and development.
Are there psychological effects or ramifications of participation at a young age? People exercise for many reasons and children are no different. The major motivation to participate in exercise or enter competitive sports is a desire to have fun (9,10,11). One study has shown that 95% of the children polled believed that having fun while participating in a sport was more important than winning; 75% would rather play on a loosing team than “sit” on a winning team (12).
Sports competition can produce severe stress and anxiety, and psychological trauma can occur when children are subjected to repeated episodes of failure in competition. Two groups of vulnerable children have been identified: those with a low level of athletic competence due to late maturation, inexperience, or genetic lack of ability, and those who perceive they are not meeting the expectations of their age/peer group, coach, or (most importantly) parents (10,13).
Seefeldt (14) offers the following “Bill of Rights” for young athletes:
The right to participate in sports.
The right to participate at a level commensurate with maturity and ability.
The right to have qualified adult leadership.
The right to play as a child and not as an adult.
The right to share in the leadership and decision-making of their particular sport.
The right to participate in a safe and healthy environment.
The right to proper preparation for participation in sport.
The right to an equal opportunity to strive for success.
The right to be treated with dignity.
The right to have fun in sports.
What are children’s norms, and how far can they drive themselves or be driven by others? This represents one of the least known and most potentially dangerous areas of sports medicine. It is an important question to ask even if it is unanswerable at present.
Can children achieve a training effect? To answer this question, we must look closely at the growth and maturation processes taking place in the pubescent individual. The “trigger hypothesis” has been used to explain specific changes and lack of changes in the physical conditioning of children. This hypothesis states that there is one critical period in a child’s development (termed the trigger point), usually coinciding with puberty, before which the effects of physical conditioning from any mode are minimal, if they occur at all. It is felt that this phenomenon is the result of the modulating effects of hormones, the same hormones that initiate puberty and influence the functional development and subsequent organic adaptations seen in the mature adult. We must be careful not to imply that prepubertal changes in conditioning do not occur. On the contrary, functional changes and adaptations are apparently as a normal consequence of the growth-maturation process (15,16). Figure 6B.2 illustrates a schematic drawing compiling data on VO2max levels of various age groups.
It has long been suspected that the ultimate limit for physiological performance is set by genetic makeup. The contribution of genetic potential to the adaptation to conditioning is major. Heredity has been shown to account for anywhere between 81% and 93% of the observed differences in cardiorespiratory endurance. Researchers who have studied the phenomenon of puberty state that certain yet-to-be-known organic adaptations involving endocrine functions must be present for puberty to occur. The trigger hypothesis (see Figure 6B.3) represents a parallel assumption that for organic adaptations for training and conditioning to occur, certain necessary conditions must precede those adaptations. An increase in lean to fat body ratio, maturation of the neuromuscular system, and increase in the levels of endocrine function must precede any significant training effect in children (17).
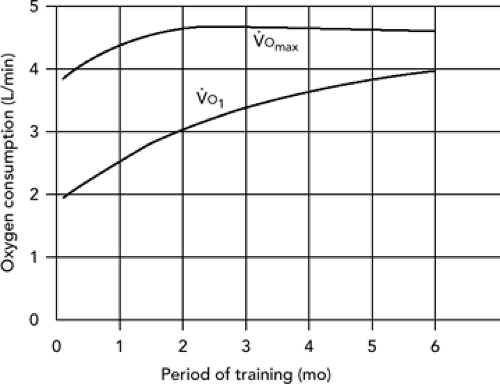 Figure 6B.1 Adaptation of body to training over time |
Both androgen and growth hormone are thought to play a part in the development of functional capacity in the pubescent individual. Androgen levels determine muscular response to resistance exercise. That response is minimal in a prepubertal youngster (18). Should a 9-year-old boy weight train? The risk (injury)–benefit (minimal muscle growth) ratio would say, “No.” Because of its many functions throughout the body, growth hormone is believed to be the prime agent working in the presence of physical conditioning to induce organic adaptations. Prepubertal athletes and nonathletes differ little in their metabolic adaptation processes, yet they can be remarkably different in athletic performance. It appears that athletic performance in this age group is more dependent upon the level of skill development than on physiological conditioning. This principle should guide the practitioner in advising prepubertal athletes on constructing an athletic training program. Additionally, the primary care physician should be well versed in the clinical use of physical maturity staging to allow for accurate assessment of the stage of puberty before formulating any exercise program (see Chapter 4, Figure 4.3).
Postpubescent Athlete
Postpubertal children require physiological conditioning along with skill training for optimal athletic performance. There does not appear to be a definitive answer about whether conditioned prepubertal children will demonstrate greater physiological changes after puberty, but there is evidence to suggest that prepubertal conditioning may prime the body to accept changes occurring in the postpubertal individual because of training. Any postpubertal individual follows predictable adult patterns concerning exercise-induced adaptations from training and conditioning.
When working with a postpubertal individual, the concept of initial level of fitness at the beginning of an exercise program is important. An individual who starts at a low level of functioning should have room for considerable improvement. For many children who are beginning their first serious exercise training, the previous consideration is important. Aerobic fitness improvements of 5% to 25% can be expected from systematic training by postpubertal individuals. In strength training, it is not unusual to see 100% to 200% improvement during the adolescent years. Physiological adaptations to exercise in the postpubescent period may be dependent upon initial levels of strength and endurance, but they can be demonstrated within 1 to 2 weeks after starting a conditioning program if the intensity is sufficient. Optimal physical conditioning in the postpubescent individual also depends upon the frequency, intensity, and duration of exercise, just as it does with adults. Most changes seen in this group result from the intensity of the training overload. Wilmore (19) indicates
that the greater the relative training intensity, the greater the training adaptation. There probably is a “minimal” threshold intensity below which training effects will not occur, as well as a possible “ceiling” threshold above which there are no further gains in adaptation. Studies of the frequency of activity in the postpubertal individual have shown that training more than 3 to 4 days a week yields very little additional change in physiological function. It appears that rest between exercise sessions is an important component in producing biological adaptations in this age group. The duration of exercise to build endurance requires a minimum of 25 to 30 minutes and an approximate 300 kcal expenditure for adaptations to take place. Strength training workouts need not exceed 40 minutes at maximum intensity levels.
that the greater the relative training intensity, the greater the training adaptation. There probably is a “minimal” threshold intensity below which training effects will not occur, as well as a possible “ceiling” threshold above which there are no further gains in adaptation. Studies of the frequency of activity in the postpubertal individual have shown that training more than 3 to 4 days a week yields very little additional change in physiological function. It appears that rest between exercise sessions is an important component in producing biological adaptations in this age group. The duration of exercise to build endurance requires a minimum of 25 to 30 minutes and an approximate 300 kcal expenditure for adaptations to take place. Strength training workouts need not exceed 40 minutes at maximum intensity levels.
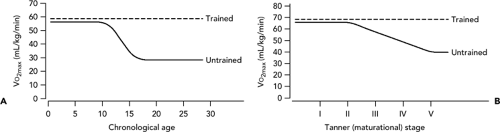 Figure 6B.2 Trigger hypothesis. A: Cardiorespiratory performance during childhood and adolescent years. Trained refers to individuals maximally trained by aerobic means, regardless of age or sex. Untrained refers to individuals whose exercise is limited to activities of daily living. B: Cardiorespiratory performance is related to maturational stage. Trained refers to individuals maximally trained by aerobic means, regardless of age or sex. Untrained refers to individuals whose exercise is limited to activities of daily living. |
Section C The Female Athlete
There has been a dramatic increase in the participation of women in physical activity in the past few decades. More women of all ages are exercising and training intensively for endurance events. More women of all ages can be seen in a variety of sports in the competitive and recreational setting. This surge in participation has raised a number of issues that pertain to the female athlete. Many relate to the female reproductive/endocrine function. Puberty may be delayed in young women involved in intensive training programs, and menstrual cycle abnormalities resulting from endurance training have been increasingly reported. These include shortened luteal phases, oligomenorrhea, amenorrhea, and anovulation. Concerns about future infertility and accelerated osteoporosis, in addition to the effects of active exercise programs on pregnancy, fetal growth retardation, and birth complications must be addressed.
It is important to look at the physical and mental makeup of the female athlete involved in exercise and sport. There are obvious physical differences between male and female athletes (see Table 6C.1) that may affect their potential for sports participation (20). However, the female can and should enjoy all the benefits of sports, exercise, and better health through active participation in a regular program.
The change in society’s attitudes toward athletic participation by women during the early 1970s, along with opportunity for older women to become actively involved in exercising, has led more female athletes to seek advice about exercise. The physical skills and knowledge about sports by women born after 1960 is vastly different from those of older women who are entering the sports world as novices. The older woman may be enthusiastic in pursuing a regular exercise program, but she lacks the rudimentary knowledge of conditioning techniques, how to select appropriate equipment and clothing, and how to protect herself from overuse and acute injuries.
Aerobic Power
Habitual level of activity, not gender or age, is the primary determinant of an individual’s cardiovascular fitness. Male and female athletes who participate in the same sport are more similar in aerobic power (VO2max) than athletes of the same sex in different sports. The elite male athlete has a higher VO2max than the elite female athlete. The lower oxygen carrying capacity of a woman, a reflection of lower hemoglobin levels, is probably the major factor in this difference. Absolute levels of VO2max usually are higher for men because males have a larger body mass than females and VO2max is directly related to body size. This presents a problem for women only in the sports or activities in which both sexes must perform at the same absolute work rate.
One of the most important concepts in all descriptive research studies is the fact that female athletes can obtain high levels of cardiovascular fitness. They are physiologically capable of undergoing the physical stress of endurance sports and they do not, as many texts imply, reach their peak fitness levels at age 15 (20). Older female athletes generally possess cardiovascular fitness levels equivalent to those of sedentary women a decade younger, whereas older women trained specifically for endurance events, gain two decades or more in fitness levels. Women who were inactive during their early adult years but now are actively engaged in physical fitness programs show significant training effects, which may improve longevity and general fitness.
Gender per se is not the factor that must be considered when prescribing exercise for women. The female’s initial level of fitness, her previous exercise experience, and her level of knowledge and skill are more important. The younger female with no previous experience in sports who wants to be in a regular exercise program will require much more guidance than a woman with prior competitive experience. The basic principles of exercise prescription outlined in this chapter apply equally to men and women. It is likely, however, that there will be greater variation in the background and experience of women seeking advice regarding exercise.
Strength
The potential of female athletes to develop strength has been greatly underestimated. Women benefit from strength training and demonstrate improved athletic performance and prevention of injury. The female athlete can obtain approximately the same kind of increase in strength as men with only a fraction of the male athlete’s increase in bulk. Increased muscle mass in men gives the male athletes a strength advantage that most women are unlikely to overcome. The anabolic properties of testosterone account for the major difference in muscle size between the sexes. In general, the overall strength of women is approximately 67% that of men. Upper body strength of the female
athletes averages approximately 65% of the male athletes, whereas leg strength is almost identical when expressed relative to body mass. The major gender differences lie in the size of the muscle fiber. Although fiber area can be increased with strength training, men still maintain an advantage in fiber size because of biological differences between the sexes.
athletes averages approximately 65% of the male athletes, whereas leg strength is almost identical when expressed relative to body mass. The major gender differences lie in the size of the muscle fiber. Although fiber area can be increased with strength training, men still maintain an advantage in fiber size because of biological differences between the sexes.
TABLE 6C.1 Physiological Differences between Men and Women and Their Effects on Athletic Performance | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||
Female athletes should not be discouraged from developing the muscular strength to meet the demands of their sport. Development of upper and lower body strength should be a priority for most female athletes. Female athletes should be encouraged to strengthen their quadriceps and hamstring muscles to prevent knee injuries.
Body Composition
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


