CHAPTER 5 Complications of Knee Arthroscopy
CLINICAL OR MEDICAL COMPLICATIONS
Deep Venous Thrombosis and Pulmonary Embolus
Deep venous thrombosis (DVT) has been reported to be as high as 17.9% after arthroscopy of the knee. Some authors have stated that without proper screening, fatal pulmonary embolus (PE) may be as high as 1.3% of cases.1 At an advanced arthroscopic knee course in August 2006, the audience was surveyed; 4 out of 40 knee arthroscopic surgeons had experienced a fatal PE in their practice, with an incidence in this small group of 10%.2 Although arthroscopy of the knee is considered to be a “benign” procedure, one study noted at least one risk factor for DVT in 37% of patients undergoing routine knee arthroscopy.3 In 2004, Geerts and colleagues4 reported on multiple risk factors contributing to DVT and PE, including obesity, history of prior DVT, cancer, use of oral contraceptives, and increased age. Anderson and Spencer5 categorized the top 10 factors causing DVT and ranked them in terms of risk. Age older than 40 years was the most significant causative factor followed by obesity, prior history of DVT, cancer, bed rest longer than 5 days, major surgery, congestive heart failure, varicose veins, hip or lower extremity fracture, and estrogen treatment. They further noted that one or more risk factors increased the incidence of development of subclinical DVT or PE to 96.3%.
Eynon and associates6 were one of the first to suggest that all patients having routine knee arthroscopies should receive anticoagulant prophylaxis. One study has reported the incidence of DVT and/or PE when comparing a control group and a second group treated with low-molecular-weight heparin (LMWH) without any known risk factors to be as high as five times greater when diagnosed by ultrasound on days 7 and 10 postoperatively.7 Another study noted a 10 times greater incidence of DVT and/or PE after preoperative and postoperative treatment with LMWH when diagnosed with ultrasound at 12 and 31 days postoperatively.8 It is estimated that between 20% to 30% of calf thrombi propagate proximally to the popliteal and femoral veins, which have an increased chance of resulting in PE. Some have argued that pharmacologic DVT prophylaxis should be routinely prescribed to patients undergoing knee arthroscopy for that reason.1,6 However, there are no agreed on recommendations in the literature about prophylaxis for arthroscopy of the knee, with or without prior history of DVT or PE.1 We recommend that all those undergoing knee arthroscopy should be given acetylsalicylic acid (ASA) preoperatively and postoperatively for 4 weeks and that those with acquired, genetic, or hemostatic risk factors be placed on preoperative and postoperative warfarin (Coumadin) or LMWH for 3 to 4 weeks to reduce the possibility of PE or DVT.
Wrong-Site Surgery
Wrong-site surgery (WSS) accounts for approximately 2% of all orthopedic claims. However, 84% result in a mean court award to the plaintiff of $48,087. Most of these were knee arthroscopies. The Physician Insurer’s of North America recorded 331 WSS claims from 1985 to 1995, and 225 were against orthopedic surgeons.9 The incidence of WSS reported to the American Academy of Orthopaedic Surgeons (AAOS) between January 1995 and December 2003 were 17% wrong knee, 12% wrong person, and 10% wrong procedure. Interestingly, hospital-based ambulatory surgery centers had the highest incidence of errors, 53%. The three most important factors to prevent wrong-site surgery errors were preoperative patient identification, surgical site indelible marking, and the physician’s signature on the surgical site. When all three of these were done, there was a 0% failure rate. However, when only two of these three were done, there was a 12% incidence of failure.10 Additional analysis of the complications that occurred estimated that an orthopedic surgeon has a 25% chance of performing wrong-site surgery during his or her career and that WSS tends to increase with increasing age and increased caseloads.9,11
In a survey presented at the AAOS in 2005, 1575 Arthroscopy Association of North America members reported an incidence of one WSS for every 26,581 arthroscopic procedures that were performed. The average age of the respondents was 48.2 years, with a practice mean of 15.8 years; 8.5% of respondents had performed wrong-site arthroscopy at least once during their careers. In this survey report, the risk of WSS increases with surgeon age, increasing years of practice, and increased surgical volume.12 In Minnesota, in 2004, there were 22 adverse events reported—13 patients had the wrong body part operated on, in four cases the wrong patient was operated on, and in five cases the wrong procedure was performed. In 2005, in Minnesota, there were 26 adverse events—16 patients had the wrong body part operated on, in two cases the wrong patient was operated on, and in eight cases the wrong procedure was performed.13
Infection
The incidence of infection after knee arthroscopy has been reported to be from 0.04% to 0.42%.14–16 Risk factors that have been reported to contribute to knee arthroscopy infections include intra-articular steroids given intraoperatively, increased surgical time, prior surgical procedures, chondroplasty, and soft tissue débridement.17 The diagnosis of infection can be difficult to make immediately postoperatively. Persistent pain and swelling after arthroscopy should have joint aspiration and culture despite the absence of fever, erythema, leukocytosis, or benign-appearing joint fluid. This diagnosis needs to be made immediately, if possible, and then treated with knee arthroscopy, lavage, and 2 to 6 weeks of intravenous antibiotics. Antibiotic prophylaxis in knee arthroscopy has been discussed and debated by several authors. Based on objective published literature, there is no statistical improvement in infection rates with preoperative IV antibiotics in routine arthroscopic surgery of the shoulder and knee.18 However, in today’s legal climate, others have argued that prophylactic antibiotics may be considered the standard of care in the local community and should be given regardless.19 Suggestions to avoid infections include operating efficiently and using antibiotic prophylaxis on immunocompromised patients. Furthermore, avoid the use of intra-articular steroids immediately prior, during, or after surgery. Finally, treat a swollen extremely painful knee postoperatively with immediate aspiration, cultures, and then aggressive arthroscopic débridement if the culture is positive, followed by IV antibiotics.
TECHNICAL OR IATROGENIC COMPLICATIONS
Nerve and Vascular Injury
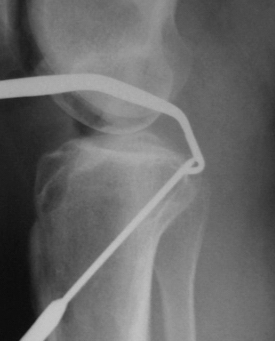
Early reported complications of meniscal repair were common; these included saphenous neuropathy medially and peroneal neuropathy laterally secondary to injury and for nerve entrapment. Other complications associated with open meniscal repair, including both outside-in and inside-out techniques, were arthrofibrosis, severe postoperative effusion, and superficial and deep infection. Combined complication rates were reported as high as 18%.20 Nerve and vascular injury have also been reported secondary to lateral meniscectomy and posterior cruciate and anterior cruciate ligament reconstruction. Despite the use of guide pins for the placement of the tibial guide pin (Fig. 5-1) during both anterior and posterior cruciate ligament reconstruction, popliteal artery injury (Fig. 5-2) continues to be of concern.21

Chondral Injury
Iatrogenic chondral injury is common during routine meniscectomy, especially in a tight medial compartment. In our experience, the presence of articular scuffing will result in significant degenerative changes within a few years and sometimes even in a few months. Note the significant chondral injury at 1 year postoperatively in a 45-year-old patient after a routine meniscectomy (Fig. 5-3). After 4 years, significant changes can occur from a routine meniscectomy (Fig. 5-4

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


