Compartment Releases of the Foot
Arthur Manoli II
David J. Dixon
INTRODUCTION
Many traumatic injuries of the foot result in severe pain and swelling (1, 2, 3, 4, 5 and 6). Multiple fractures and/or dislocations and fractures as a result of high-energy injuries (calcaneal fractures) may produce blood and interstitial fluid accumulation within the rigid, fascial confines of the compartments of the foot. As seen in compartment syndromes elsewhere in the body, the pressure built up in the compartments may result in muscle ischemia and necrosis with subsequent scar formation, and the formation of contractures of the soft tissues (7). This will often result in marked dysfunction of the foot with frequent sequelae including claw toes, chronic pain, stiffness, and nerve dysfunction. Early fasciotomy, performed emergently after the diagnosis of foot compartment syndrome is made, minimizes the chance of developing late contracture, nerve dysfunction, and disability (8, 9 and 10).
INDICATIONS AND CONTRAINDICATIONS
Severe injuries of the foot, particularly those with multiple fractures or an element of crushing, are prone to develop foot compartment syndrome. Tense foot swelling that develops after an injury should alert the practitioner to the possibility of a compartment syndrome. Plantar foot ecchymosis is often present (Fig. 29.1). Severe pain, pain with passive stretch of the foot muscles (toe dorsiflexion stretches the plantar muscles), and nerve dysfunction (paresthesias, muscle paralysis) may be seen, but are thought to be less diagnostic in the foot than elsewhere. The direct measurement of compartment pressures is suggested in suspicious instances to confirm the diagnosis of foot compartment syndrome (11, 12 and 13). There should be a low threshold for measuring the foot compartment pressures in clinically suspicious cases, particularly those associated with severe injury, that is, crush, and in unconscious patients (14). The presence or absence of the peripheral pulses is of no use in diagnosing foot compartment syndrome.
Severe pain out of proportion
Tense foot swelling
Plantar foot ecchymosis
Pain with passive stretch
Inability or difficulty moving toes
Low threshold for measurement of compartment pressures
PREOPERATIVE PLANNING
Catheterization of the nine compartments of the foot can be done using any of the well-known established apparatuses (8,15, 16 and 17). The development of portable pressure monitors (Pressure Sense Monitor, Ace Medical Co., Los Angeles, CA, or Digital Quickset, Stryker Corp., Kalamazoo, MI) has made the measurement of pressures much easier. They may be performed almost anywhere with ease and accuracy.
 FIGURE 29.1 Clinical appearance of tense foot swelling in compartment syndrome following calcaneal fracture with plantar ecchymosis, plantar view. |
The pressures within the compartments of the foot may be measured using local, infiltrative anesthesia (Fig. 29.2). Medial compartmental pressure is measured with a stick approximately 4 cm inferior to the medial malleolus, over the abductor hallucis muscle (Fig. 29.3A). Advance the needle through the medial intermuscular septum of the foot into the deep hindfoot compartment, the calcaneal. Here, the pressure is often found to be the highest, especially in the instances of calcaneal fractures. The needle is removed and reinserted into the flexor digitorum brevis muscle in the arch, measuring the superficial compartment (Fig. 29.3B). A third stick, on the lateral aspect of the foot, just below the fifth metatarsal, measures the pressure in the lateral compartment (Fig. 29.3C). Any or all of the separate interosseous compartments can be sampled in the forefoot. It is recommended that at least one of the first and second interosseous compartments be measured (Fig. 29.3D). Here, if the needle is advanced deeply between the respective metatarsals, the pressure in the adductor compartment can also be measured.
Although the absolute pressure at which fasciotomy should be performed continues to be an unknown, normal pressures are known, and certain guidelines have been developed for abnormal pressures. Dayton et al. (15) reported that normal compartment pressures in the foot are less than 6 mm Hg. Capillary vessel wall closing pressure is around 30 mm Hg (16). Some authors recommend performing a fasciotomy for intracompartmental pressures exceeding 30 mm Hg. Whitesides et al. (17) suggest that they be performed for pressures greater than 30 mm Hg below diastolic blood pressure. Schneck et al.’s (7) study has indicated that metabolic dysfunction is severe when the pressure exceeds 30 to 40 mm Hg below mean arterial pressure.
Certainly the patient’s injury severity, overall metabolic status, circulatory status (blood pressure and pulse), and the clinical evaluation must also be considered. Hypotensive patients, usually from polytrauma, generally have a greater risk of developing compartmental syndromes at lower pressures. The duration of increased pressure and pressure trends may be helpful. Unconscious patients with foot injuries should also be observed closely; if suspicious, compartment pressures should be obtained.
Of the nine compartments of the foot, the calcaneal compartment, which lies deepest in the foot adjacent to the calcaneus, is the most often involved compartment following calcaneus fractures (Fig. 29.4) (18). Up to 10% of calcaneus fractures develop compartment syndrome of the foot (9,19). Interosseous and adductor compartment syndromes are reported to occur following Lisfranc and Chopart joint injuries and crush injuries to the forefoot (14). Isolated medial foot compartment syndrome (abductor hallucis muscle) has been reported as an exertional syndrome in athletes (1), and as an isolated syndrome occurring idiopathically without injury (20). Concurrent compartment syndromes of the leg and foot have been reported and are probably associated with communication between the deep posterior compartment of the leg and the deep compartments of the foot (20). Although not reported, it may be important to consider release of the foot compartments, as is done in the leg compartments to prevent reperfusion compartment syndrome, following vascular reconstruction of the lower extremity large vessels.
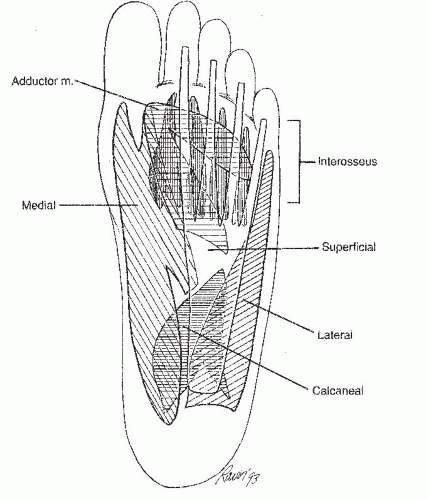 FIGURE 29.2 A plantar view of the nine compartments of the foot. The medial, superficial, and lateral run the entire length of the foot. The adductor and four interosseous compartments are located only in the forefoot. The calcaneal compartment is situated in the hindfoot. (Adapted from Manoli A II, Fakhouri AJ, Weber TG. Compartment catheterization and fasciotomy of the foot. Oper Tech Orthop 2:203-210, 1992.) |
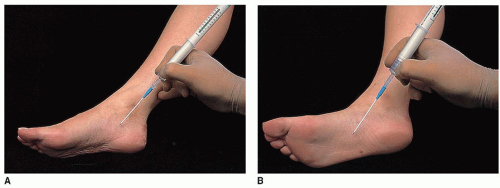 FIGURE 29.3 A: A medial stick, 4 cm below the medial malleolus, to measure the pressure in the medial and calcaneal compartments. B: On the plantar surface of the foot, in the arch area, the superficial compartmental pressure is measured. This compartment contains the flexor digitorum brevis muscle. |
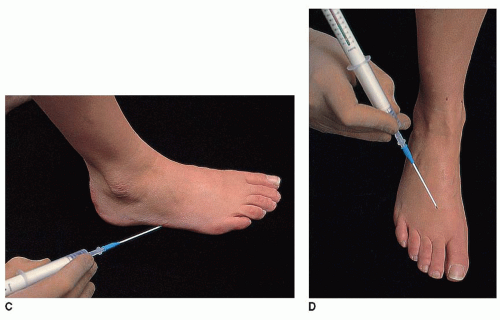 FIGURE 29.3 (Continued) C: The lateral stick is just below the fifth metatarsal base to measure the pressure in the lateral compartment. D: A stick in the first or second interspace to measure the pressure in that space. Advancement of the needle deeper into the forefoot to measure the pressure in the adductor compartment. |
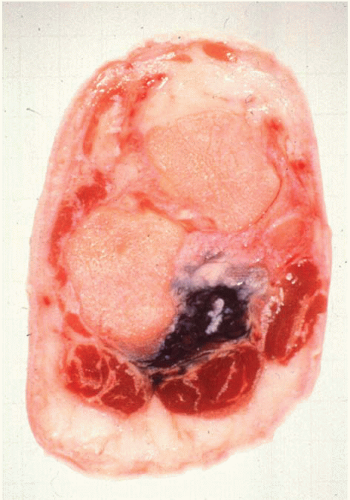 FIGURE 29.4 An ink injection study illustrating the fascial confines of the calcaneal compartment (dark), superficial plantar compartment (plantar to calcaneal compartment), medial compartment, and lateral compartment. The neurovascular bundle is adjacent to medial fascia in calcaneal compartment. (From Manoli A II, Fakhouri AJ, Weber TG. Fasciotomy of the foot: an anatomical study with special reference to release of the calcaneal compartment. Foot Ankle 10:267-275, 1990.) |
Related posts:
 Oblique First Metatarsal Osteotomy: Ludloff
Intramedullary Screw Fixation of Jones Fractures of the Fifth Metatarsal
Metatarsal and Calcaneal Osteotomies for Cavus Foot
Tibiofibular Syndesmosis Reduction and Fixation
Arthroscopic Treatment of Ankle Osteophytes and Osteochondral Lesions of the Talus
Osteochondral Autologous Transfer Procedure for Repairing Articular Cartilage Defects in the Talus: OATS Procedure
Oblique First Metatarsal Osteotomy: Ludloff
Intramedullary Screw Fixation of Jones Fractures of the Fifth Metatarsal
Metatarsal and Calcaneal Osteotomies for Cavus Foot
Tibiofibular Syndesmosis Reduction and Fixation
Arthroscopic Treatment of Ankle Osteophytes and Osteochondral Lesions of the Talus
Osteochondral Autologous Transfer Procedure for Repairing Articular Cartilage Defects in the Talus: OATS Procedure
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


