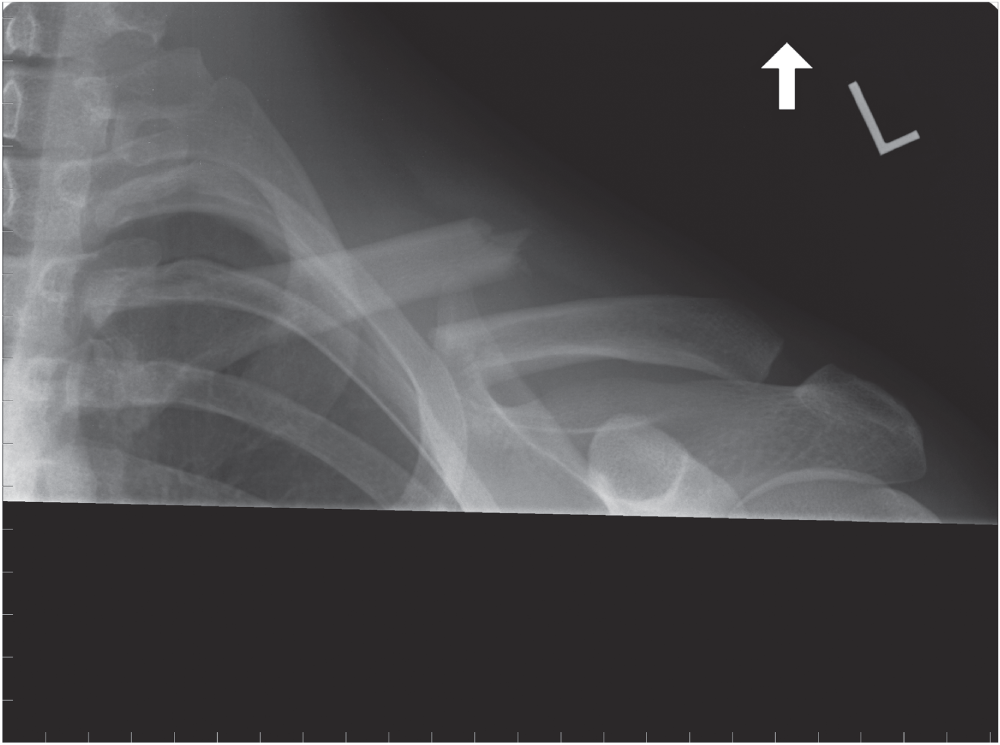
Chad Myeroff MD and Michael D. McKee MD FRCS(C) University of Minnesota, Department of Orthopaedic Surgery, Regions Hospital and TRIA Orthopedic Center, St Paul, MN, USA Department of Orthopaedic Surgery, University of Arizona College of Medicine, Phoenix, AZ, USA Figure 78.1 Radiograph of a 30‐year‐old man who fell off his mountain bike and sustained a midshaft clavicle fracture. Displacement and shortening is evident. In order to optimize care, it is important to identify the minority of patients who are at risk for poor outcomes with nonoperative management. Nonoperative management is not without risks, so physicians and patients should understand fracture and patient characteristics that negatively affect the outcome in nonoperatively treated fractures. After searching the literature, nine studies were utilized to answer this question including: two level I studies and further supported with level II–IV data. The majority of patients with a clavicle fracture will heal uneventfully with satisfactory function with nonoperative treatment. However, a minority of patients will have ongoing sequelae from a displaced midshaft clavicle fracture as shown in a recent randomized clinical trial (RCT) reporting 23.1% nonunion with nonoperative management of midshaft displaced fractures.1 In addition to the unexpected 15% nonunion rate reported by Hill in 1997, a 31% dissatisfaction rate, related to 25% of patients complaining of deformity and a 29% incidence of thoracic outlet syndrome, was reported. They found initial shortening >2 cm was significantly associated with nonunion and unsatisfactory results (p <0.0001).2 McKee looked at 30 healed, displaced fractures using patient‐based outcomes and strength testing. They showed 27% dissatisfaction, Constant score of 71, and a Disabilities of the Arm, Shoulder, and Hand (DASH) score of 25. There was a trend toward worse DASH scores for shortening >2 cm and there was a statistically significant inverse correlation between abduction endurance strength and shortening.3 Lazarides found a 25.8% dissatisfaction rate in patients with a healed midshaft clavicle fracture, significantly associated with shortening >18 mm in males and >14 mm in females.4 This phenomenon has recently been challenged by Goudie, but with an average of only 11 mm shortening and only five patients with >2 cm shortening, this study was underpowered to detect a statistical difference.5 In a systematic review, Zlowodzki reported an overall nonunion rate of 5.9% which increased to 15.1% for completely displaced fractures.6 Robinson’s study employing multivariate analysis found increasing fracture displacement, comminution, advancing age, and female gender all to be independent predictors of nonunion in shaft fractures.7 Nowak also found that displacement, comminution, and older age were predictors for sequelae (pain and deformity) following clavicle fracture.8 Murray reviewed 941 diaphyseal fractures managed nonoperatively and identified smoking (odds ratio [OR] = 3.76; 95% confidence interval [CI]: 2.39–5.89; p <0.001), displacement (OR = 1.17; 95% CI: 1.13–1.21; p <0.001), and comminution (OR = 1.75; 95% CI: 1.11–2.76; p = 0.015) to be statistically significant risk factors for nonunion.9 Multiple high‐quality RCTs have suggested potential benefits to primary operative fixation of displaced midshaft clavicle fractures. Shared clinical decision‐making between patient and provider demand an unbiased, accurate understanding and communication of the literature. After searching the literature, 11 studies were utilized to answer this question. Of these, six were level I studies including multiple high‐quality RCTs. Zlowodzki et al. performed a systematic review of 2144 clavicle fractures. In a subset analysis of only displaced fractures, 460 plated fractures had a nonunion rate of 2.2% versus 15.1% for nonoperatively treated displaced fractures. They reported a nonoperative relative risk (RR) 6.9 (95% CI: 3.4–14.2) for nonunion and an absolute risk reduction (ARR) OF 12.9%, with a number need to treat of 7.8 patients to avoid one nonunion for plating; relative risk reduction (RRR) of 86% (95% CI: 71–93%; p <0.001).6 In 2007, an RCT comparing plate fixation versus nonoperative treatment for displaced midshaft clavicle fractures demonstrated statistically significant differences including a shorter time to union (16.4 vs 28.4 weeks; p = 0.001), improved Constant and DASH scores, as well as improved patient satisfaction (p = 0.002) and appearance (p = 0.001) in the operative arm.10 Complications for the operative group were 37% versus 63% for nonoperative treatment. The operative group’s complications included hardware irritation, removal of hardware (ROH), transient brachial plexus irritations, and wound complications (4.8%). The nonoperative group had complications predominated by nonunion (7/49; 14.3%), malunion requiring corrective surgery (9/49; 18.4%), and brachial plexus irritation. The only statistically significant difference in complications were lower nonunion (15% vs 3.2%; p = 0.04) and malunion (22.5% vs 0%; p = 0.001) in the operative group.10 Smith and Smekal noted similar results following operative fixation of displaced midshaft clavicle fractures in two other RCTs.11,12
78
Clavicle Fractures
Clinical scenario
Top three questions
Question 1: In patients with clavicle fractures managed nonoperatively, do displaced fractures have worse outcomes than nondisplaced fractures?
Rationale
Clinical comment
Available literature and quality of the evidence
Findings
Resolution of clinical scenario
Question 2: In patients with displaced clavicle fractures, does open reduction and internal fixation offer improved outcomes compared to nonoperative management?
Rationale
Clinical importance
Available literature and quality of the evidence
Findings
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


