Fig. 3.1
Effect on overuse injury occurrence due to the theoretical relationship between stress application and frequency (According to Hreljac and Ferber [18])
Repeating the same movement numerous times applies stress to the body; as a consequence, the involved tissue adapts by strengthening and thickening. If the applied stress becomes too great and the body system is not able to recover and adapt quickly enough, this overload to the system leads to microtraumatic injuries, which cause inflammation of the affected area, resulting in an overuse injury as a direct response. Signs of overuse or inflammation include swelling, warmth, redness, or impaired function of the body part. Some or all of these signs may be present but not noticeable initially. Different classification systems that include four [4] to six stages [8] exist to define overuse injuries. In the four-stage system, the early stage of an overuse injury is discomfort that disappears during warm-up; the first sign is often stiffness or soreness. Continued use may cause further damage, leading to lasting pain through and beyond the warm-up and may worsen after finishing the activity. The third stage occurs when the discomfort gets worse during the activity. In the last stage, there is pain or discomfort all the time. Curwin and Stanish [8] distinguished six stages ranging from level 1, defined as having no pain and a normal level of sports performance, to level 6, which is characterized by pain during daily activities and an inability to perform in any sports. Increasing levels increase the description of pain and decreases the ability to perform any activity (Fig. 3.2).
There are several predisposing factors leading to overuse injuries of the musculoskeletal system, which consist of internal (intrinsic) and external (extrinsic) risk factors listed below (Fig. 3.3):
3.3 Pathophysiology of Overload Damage
In contrast to traumatic injury, which is defined as injury resulting from a specific, identifiable event, overuse injury is caused by repeated microtrauma without a single, identifiable event that is responsible for the injury [3]. Classification of an injury as acute or overuse is obvious in most cases, but it is sometimes more difficult, particularly when the symptoms appear suddenly even though the injury is the result of a long-term process [3]. For instance, a stress fracture is caused by overuse over time [3]. Overload damage is the sum of repetitive force and the repeated load that affects the tissue. This process leads to microtraumas that excite the inflammatory response (Fig. 3.4).

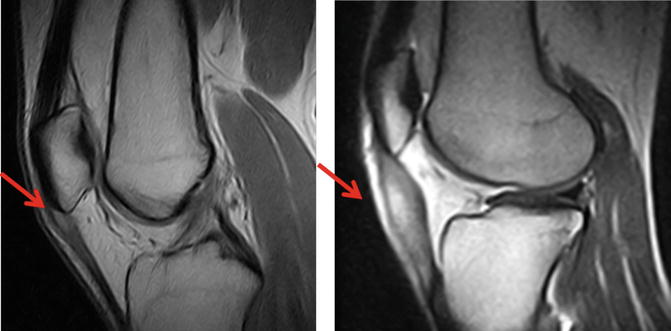
Fig. 3.4
Bone marrow edema of the medial tibial condyle due to overuse in a 17-year-old football player. Red Arrow indicate the injury/damaged tissue
Chronic overuse injury is a multifactorial process with many other factors such as local hypoxia, diminished nutrition, impaired metabolism, and local inflammation that may also contribute to the development of tissue damage [23]. Although it is discussed in the literature whether the pathogenesis of an overuse injury is due to inflammation or degeneration [1], injured tissue reacts with an inflammatory process, leading to a number of changes in the vascular net, blood, and connective tissue [32]. Pecina and Bojanic identify the inflammatory process as the primary cause of overuse injury, leading to degenerative changes during the course of its chronic stages [32]. If the inflammation is not fully cured, reinflammation may occur, which subsequently leads to chronic complaints. The pathophysiology of overload damage is a dynamic process, and overuse injuries are caused by repetitive, low-grade forces exceeding the tolerance of the tissues. The tissue can repair the damage without demonstrable clinical symptoms in most cases; however, in some cases, a permanent repeated workload meets or exceeds the ability of the tissue to repair and adapt, resulting in damage that leads to the symptoms of an overuse injury [45]. These repetitive microtraumas are the result of repeated exposure of the musculoskeletal tissue to low-magnitude forces [22], and this microtraumatic response is the failed adaption to physical load and use [32]. These effects are chronic and cumulate in microtraumatic injury [32]. For example, most elbow injuries result not from acute trauma but from repetitive microtrauma and chronic stress overload of the joint (Fig. 3.5) [31].
3.4 Physical Constitution
The desired goal of improved performance is reached by prescribed periods of intense activity. During these periods of intense activity, stress is applied to the body. During periods of rest and recovery, the involved tissue adapts by strengthening and thickening. However, a mismatch between overload and recovery may lead to a breakdown on a cellular, extracellular, or systemic level [44]. Being a beginner to sports or starting again after a hiatus often accompanies poor preparation and/or inadequate conditioning that can substantially increase the incidence of overuse injuries [32]. This is often the case in young athletes, especially when they are beginners or in older athletes who want to restart training at an athletic level attained some time before the training interruption. Tissue breakdown and overuse injury is then the direct response at the cellular level when tissue that fails to adapt to new or increased demands is exposed to repetitive overload. Even before the person experiences pain and becomes symptomatic, subclinical tissue damage might have occurred. Rapid increases in training load and inadequate recovery may cause global overtraining syndrome at the systemic level [44].
Dye et al. classified four different zones of loading across a joint (see Fig. 3.6): the zone of subphysiological underload; the zone of homeostasis, which is limited through the envelope of function; the zone of supraphysiological overload; and the zone of structural failure [9]. Training load around the area of the envelope of function leads to adaptive processes that make tissues stronger and thicker, leading to enlargement of the zone of homeostasis; the envelope of function widens, and the athlete is able to perform under higher loads or achieve longer durations of physical activity. High load, high frequency, or combined overloading over a period of time pushes the body systems into the zone of supraphysiological overload or even structural failure, which subsequently leads to an injury. The zone of subphysiological underload affects an injured athlete who is not able to train or perform in any physical activity, causing catabolic processes, e.g., when extremities must be immobilized to support healing and therefore cannot be moved. In the same way that the envelope of function widens through training load, insufficient stimuli or injury decreases the envelope of function, and the zone of homeostasis is reduced. If an athlete returns to sports after an injury or a long period of inactivity, the envelope of function is lower than before and is likely significantly lower than recognized by the athlete. Returning to sports and restarting the prior training volume at which the athlete was accustomed to performing might exceed the envelope of function due to poorer physical constitution as a consequence of training interruption.
3.5 Gender Differences
There are differences between genders in the context of anatomic, physiologic, and psychological aspects [32]. Although athletic injuries seem to be sports rather than gender related [32], male athletes seem to have a higher risk of severe sports-related injuries [35], while women are more affected by overuse injury than men [6, 14, 37]. A study by Yang et al. revealed “that more than one-quarter of all injuries sustained by collegiate athletes were overuse injuries, with female athletes having a higher rate of overuse injuries than male athletes” [46]. Gender differences in the incidence of patellofemoral pain syndrome lead to a rate of 20 % in women versus 7.4 % in men, while the risk of repeated patellar dislocation is six times higher in women than in men [32]. Relative to body weight, women’s limbs are shorter and smaller than those of men. Smaller bones are less powerful levers; additionally, women have a wider Q angle, which is a predisposing factor for patellofemoral problems [32]. Men have greater muscle mass than women [7, 20, 40], and women have decreased muscle-to-strength ratios between the quadriceps and hamstrings relative to men [32, 40]. As such, relative muscle weakness may be a risk factor for overuse injuries. Frequently conducted strength training to increase muscle power has been shown to decrease overuse injuries in the lower extremities of female recruits [33]. There are differences in muscle activity in response to anterior tibial translation, as female athletes use their quadriceps muscle, while male athletes and sex-matched nonathletic people rely more on their hamstring muscles for initial knee stabilization [19]. Increased ligamentous laxity is a widely accepted belief that is only partially true, while the role of cyclical estrogen and progesterone production has yet to be determined [32]. However, menstrual status among female athletes is considered to represent a risk factor for overuse injury [29, 36]. In young female athletes, intense training is often accompanied with low caloric intake, leading to amenorrhea or delayed menarche [28] that “may lead to hypoestrogenism and a decrease in bone material content predisposing these athletes to stress fractures” [32].
3.6 Mental Influences and Psychological Factors
Athletes who suffer overuse injury often mention psychological factors as a cause for their injury, e.g., “having too much of a drive,” “wanting to succeed,” “not knowing when to stop,” and “training despite being fatigued” [45]. In certain sports such as high-performance bodybuilding, it seems that pain is accepted as part of the sports. Although the injury rate is low, a large number of athletes complain of pain or problems during routine workouts. High levels of motivation, discipline, and willpower may explain this phenomenon [39]. There is growing evidence that athletes’ psychological characteristics are important for understanding overuse injuries in sports [42]. In a study by Timpka et al., 68 % of athletes reported an injury during the study period. Of these reported injuries, 96 % were classified as being associated with overuse [42]. Injury risk is increased by maladaptive coping through self-blame and hyperactivity [42]. Male adult athletes with previous serious injuries also showed an increased risk of injury, while the injury risk was decreased for male and female adult athletes without previous injury [42]. This finding may lead to the assumption that male athletes consider their body to be a tool that must function; training too hard and not granting the body enough rest during injury are more of a risk factor that can be attributed to male athletes. Attentiveness and care for the body during injury periods may decrease the risk of re-injury. The psychological factors of self-blame and hyperactivity, combined with previous injury, age, and gender, are considered to be risk factors for overuse injuries in athletes [42]. Not only should physical forces be considered but the importance of psychological factors and social context must be included as well because “an athlete with high physical demands may be more likely to suffer an overuse injury if she also feels herself to be in a stressful situation” [45]. If athletes return to sports after an injury, it has been shown that they experience injury-related distress although they are physically recovered from their injuries [43].
3.7 Excessive Work in Training and Competition
Sudden increases in training volume and changes in the type of training, especially running, are considered to be risk factors for overuse injury [32]. Achilles tendinopathy is the most common overuse injury in runners, followed by runner’s knee, plantar fasciitis, and shin splints [25]. Knobloch et al. showed that running more than four times a week or an exposure for more than 2600 km led to a higher risk of shin splint overuse injuries. Runners with more than 10 years of experience had a higher risk of overuse injuries of the back and Achilles tendinopathy; training more than 65 km/week increased the risk for back overuse injuries [25]. Male runners over 35 years of age are more often prone to these complaints, especially after they have intensified their training routine with interval runs on the track or threshold runs (Fig. 3.7) [24].
 General Prevention Principles of Injuries
Special Aspects of Prevention in Children and Adolescents
Implementation of Prevention in Sports
General Training Aspects in Consideration of Prevention in Sports
General Prevention Principles of Overload Damage in Sports
Specific Aspects of Throwing Sports in Recreational and Competitive Sport
General Prevention Principles of Injuries
Special Aspects of Prevention in Children and Adolescents
Implementation of Prevention in Sports
General Training Aspects in Consideration of Prevention in Sports
General Prevention Principles of Overload Damage in Sports
Specific Aspects of Throwing Sports in Recreational and Competitive Sport




Related posts:
General Prevention Principles of Injuries
Special Aspects of Prevention in Children and Adolescents
Implementation of Prevention in Sports
General Training Aspects in Consideration of Prevention in Sports
General Prevention Principles of Overload Damage in Sports
Specific Aspects of Throwing Sports in Recreational and Competitive Sport
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
