5 Canadian model of occupational performance and engagement
Major concepts and definitions of terms
As with the three models presented in the previous chapter, the Canadian Model of Occupational Performance and Engagement (CMOP-E) aims to make explicit the relationship between person, environment and occupation. It is based on the assumption that occupation, the domain of concern for occupational therapists, is the “bridge that connects person and environment” (p. 23). The model is presented within a larger text entitled Enabling Occupation II: Advancing an Occupational Therapy Vision for Health, Well-being and Justice through Occupation (Townsend & Polatajko, 2007). Consequently, many of the assumptions that underpin the model are embedded within the larger text.
The three main components of the model are person, occupation and environment. With reference to the diagram (Figure 5.1), these three components were described by Polatajko et al. (2007, p. 23) as follows:
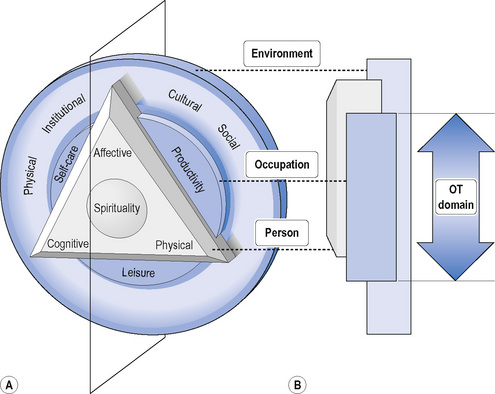
FIG 5.1 The Canadian Model of Occupational Performance and Engagement (CMOP-E).
From Elizabeth A. Townsend & Helene J. Polatajko, Enabling occupation II: Advancing an occupational therapy vision for health, well-being and justice through occupation, 2007. Reprinted with the permission of CAOT Publications ACE, Ottawa, Ontario, Canada.
This description shows that occupation is conceptualized as the agent through which person and occupation interact; portrayed as a bridge. This metaphor conjures the image of person and environment being two distinct entities that are connected through occupation, in the same way that two sides of a river are linked by a bridge. This conceptualization of person and environment as separate entities is similar to the understanding of person and environment in the PEOP model, but differs from the Person-Environment-Occupation model (Law et al., 1996) and Ecology of Human Performance (Dunn et al., 1994), reviewed in the previous chapter, with their transactive or ecological understandings of the relationship between person and environment.
Townsend and Polatajko (2007) presented six basic assumptions that underpin the model. The first two assumptions are based on the work of early occupational therapy writers such as Dunton and Howland and proposed that: (1) humans are occupational beings; and (2) occupation has therapeutic potential. The next three assumptions are that occupation: (3) affects health and well-being; (4) organizes time and brings structure to living; and (5) brings meaning to life through the combination of cultural and individual influences on the creation of meaning. The final assumption is that: (6) occupations are idiosyncratic, in that the specific occupations that a person might engage in will vary from person to person. The authors also clarified that this final assumption qualifies the earlier assumption that occupation affects health and well-being, in that this influence is not always positive; for example, occupations such as drug taking and vandalism can have a negative influence on the person or others.
In Enabling Occupation II, occupation was presented as the domain of concern of occupational therapy and an earlier definition of occupation was retained for this edition. Occupation was defined as “groups of activities and tasks of everyday life, named, organized, and given value and meaning by individuals and a culture. Occupation is everything people do to occupy themselves, including looking after themselves (self-care), enjoying life (leisure), and contributing to the social and economic fabric of their communities (productivity)” (CAOT, 1997, cited in Polatajko et al., 2007, p. 17.). Polatajko et al. emphasized that this definition, which would be consistent with most current occupational therapy understandings of occupation, represents a broader concept of the term than both the profession’s earlier notion of “occupying the invalid” (p. 17) and the general public’s association of occupation with vocation and the means of earning a living. Current occupational therapy notions of occupation refer to all forms of human action that are grouped and have meaning for individuals and cultures. The influence of the occupational performance model on CMOP-E is clear in its classification of the purpose of occupation into the three categories of self-care, productivity and leisure, although this definition of productivity could be seen as relatively broad in that it explicitly refers to the “social and economic fabric” of communities. It is also evident through the term performance components.
As the name suggests, the CMOP-E is a model of occupational performance, which is defined as “the dynamic interaction of person, occupation and environment” (Polatajko et al., 2007, p. 23). As the authors explained, the construct of occupational performance is not made explicit in the model but is foundational to and embedded within the model. To use the metaphor we introduced earlier, it is like a window through which one might look rather than a perspective in which the process of looking through the window is described. In the first approach, the window frames what you see but might not be a feature of what you are aware of or describe.
Occupational engagement and client-centred practice
The CMOP-E proposes that occupational therapy practice requires both enablement and client-centred practice. While the concept of occupational performance remains implicit in the model during its development from the Canadian Model of Occupational Performance (CMOP) (CAOT, 1997) to the CMOP-E (Polatajko et al., 2007), the authors also emphasized that the newer version of this model is not restricted to a focus on occupational performance but also encompasses the concept of occupational engagement. In explaining this difference, Polatajko et al. (2007) provided a story about a father and son who participated in marathons together. Their first run together occurred because one of the son’s classmates became paralyzed and the school organized a charity run to raise money. The son expressed a strong desire to participate. This event was the start of an occupation that father and son shared for more than four decades. The father ran, pushing his son, severely disabled from birth and only able to communicate using assistive technology operated by his head, in a wheelchair. Over the years they completed a number of marathons, 212 triathlons (in which the son sat in a dinghy and was pulled by the father while he swam) and four ironman events together. These activities had meaning for both of them. After the initial charity run, the son had commented to the father how much he had enjoyed the event because he “didn’t feel disabled” (Polatajko et al., 2007, p. 25).This, in turn, motivated the father to pursue subsequent opportunities to participate in the activity together. The “awesome feeling” he gets seeing his son smile is the reason the father does these events (p. 25). The authors used this story to illustrate that occupational performance is a more limited concept than occupational engagement, in that the son did not perform the occupation but engaged in it fully.
This story also illustrates the importance of the second major proposition in Enabling Occupation II; that enablement through occupation is the current core of occupational therapy. The authors proposed that this focus contrasted with the initial concern of the profession of “the provision of diversional activity” and with the following period in which attention centred on “the use of therapeutic activity” (Polatajko et al., 2007, p. 15). Townsend et al. (2007) reminded readers that enabling occupation had been defined in 1997 as “enabling people to choose, organize, and perform those occupations they find useful and meaningful in their environment” (p. 89). At the time this definition was originally published, choosing and organizing would probably have been considered tasks required to prepare for occupational performance. The newer definition of occupational therapy is based on the assertion that occupational therapists enable through occupation (Townsend et al., 2007). It reads:
The dictionary definition provided by Townsend et al. (2007) for the word enable refers to concepts of giving power, strengthening, providing with the ability or means to do something and with the means to do or be something, and making something possible. The definition of occupational therapy provided by the authors emphasizes three types of undertaking that are enabled: (a) people’s engagement in everyday life; (b) their performance of occupation; and (c) the development of a just society in which people can participate. For an occupational therapist to enable all three of these outcomes, their practice would need to be aimed at both personal and societal levels.
In recognition of the need to target both personal and societal levels, Townsend et al. (2007) identified six “categories of client” (p. 96) – individuals, families, groups, communities, organizations (including e.g. agencies, clubs and associations, and other government, corporate or non-government organizations) and populations. The authors stated that these categories evolved from four categories presented in the 1997 edition and this expanded view represents a practice that goes beyond working with individuals and might focus on the environment at the levels of client communities, organizations and populations. Detailed definitions of each of these client groups are provided on page 97 of Enabling Occupation II.
Client-centred practice is also fundamental to CMOP-E. Townsend et al. (2007) commented that client-centred practice means “focusing on client goals and projected outcomes” (p. 98) and pointed out that the following definition, provided in the 1997 edition of Enabling Occupation, had concepts of client-centred practice embedded within it. “Enabling is the basis of occupational therapy’s client-centred practice and a foundation for client empowerment and justice” (cited in 2007, p. 99). The assumption at the core of both enablement and client-centred practice is that occupational therapy involves “collaborating with people – rather than doing things to or for them” (p. 98). This statement needs to be understood in contrast to a biomedical approach in which ‘patients’ were primarily expected to be passive recipients of care or curative methods, rather than active participants in the process. Therefore, there might be things that client-centred and enabling occupational therapists do for people, such as advocate on their behalf for certain outcomes. However, these do not conjure the image of the passive patient.
Townsend et al. (2007) also noted that there has been a burgeoning of occupational therapy research around the notion of client-centred practice, which has not always “specifi[ed] the connection to enablement” (p. 99). However, the CMOP-E appears to assume a mutual relationship between the two concepts. This is evidenced in the statement, “In occupational therapy, client-centred practice delimits the definition of enablement; conversely enablement delimits the definition of client-centred practice” (Townsend et al., 2007, p. 99). The authors also stated that the challenges to client-centred practice are similar to those of enablement in that they can be encountered at the levels of the client and/or therapist and the broader systems surrounding them. Examples include the client’s culture and level of education, the therapist’s capacity to share power and recognize client expertise, and the management philosophies and resource distribution of the broader system.
Canadian Practice Process Framework (CPPF)
Craik et al. (2007) stated that the CPPF for occupational therapy is “a process framework for evidence-based, client-centred occupational enablement” (p. 233). This framework seems to have been developed in response to the feedback obtained regarding the Occupational Performance Process Model (OPPM), published by Fearing et al. (1997), which was seen to be “useful to guide individualized practice” (pp. 231–232) but not designed for nor appropriate to practice with “community, organization, or population clients” (p. 232). In contrast, Craik et al. proposed that the CPPF can be used with all six categories of client discussed earlier in relation to enablement. The diagrammatic representation of the CPPF is presented in Figure 5.2.
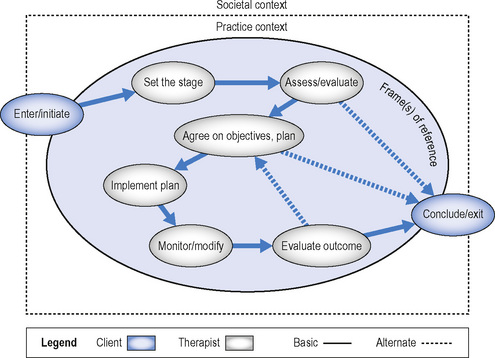
FIG 5.2 The Canadian Practice Process Framework (CPPF).
From Elizabeth A. Townsend & Helene J. Polatajko, Enabling occupation II: Advancing an occupational therapy vision for health, well-being and justice through occupation, 2007. Reprinted with the permission of CAOT Publications ACE, Ottawa, Ontario, Canada.
As Craik et al. (2007) stated, “The CPPF guides the therapist through a process of occupation-based, evidence-based, and client-centred practice, which is directed towards enabling change in occupational performance and engagement. By utilizing the CPPF, an occupational therapist would identify eight key actions in enabling any type of client to reach occupational goals.” (p. 234.) These key action points include the commencement and conclusion of the process (called enter/initiate and conclude/exit) and six other general process points. These general points are: set the stage; assess/evaluate; agree on objectives, plans; implement plan; monitor/modify; and evaluate outcome.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


